Abstract
Background. Tension gastrothorax is a rare life-threatening condition that occurs when the stomach is herniated into the thoracic cavity, most often through the congenital left posterolateral diaphragmatic defect, causing a mediastinal shift when distended with gas and fluid.
Case Presentation. A previously healthy 2-year-old boy was admitted with acute abdominal pain, vomiting and dyspnea. Chest X-ray was initially interpreted as hydropneumothorax, but after careful observation the decision was made to insert a nasogastric tube and to perform a computerized tomography scan to confirm the suspicion of tension gastrothorax. Laparotomy was performed the following day, organs were repositioned into the abdomen and reconstruction of the left hemidiaphragm was conducted.
Conclusion. When symptoms of respiratory distress occur in an otherwise healthy child, tension gastrothorax should be on the list of differential diagnosis. It is important to recognize distinct radiographic features of this life-threatening condition in order to promptly manage it. Initial placement of nasogastric tube for decompression should be followed by the reduction of the organs into the abdomen and diaphragmatic repair.
Keywords: tension gastrothorax, congenital diaphragmatic hernia, children
Introduction
Approximately 90% of congenital diaphragmatic hernias (CDH) are diagnosed with prenatal imaging or within the first 24 hours after birth. The ones that present later have a better prognosis because there is no pulmonary hypoplasia or hypertension.1 Late-onset CDH has a variety of clinical presentations and one of them is a rare life threatening condition - tension gastrothorax. Horst et al.2 showed an incidence of 5.1% (5/98) CDH presenting as tension gastrothorax in a 13 year period. It is caused by herniation of the stomach into the thoracic cavity, most often through the congenital left posterolateral diaphragmatic defect. When the stomach is significantly distended with gas and fluid it causes a mediastinal shift which can often be misinterpreted as tension pneumothorax leading to incorrect management with increased morbidity and mortality.3,4
The aim of this case report is to present typical clinical and radiographic features of tension gastrothorax and suggest the best treatment options for this rare and potentially fatal condition.
Case presentation
A previously healthy 2-year-old boy was admitted to our hospital with acute abdominal pain, vomiting and dyspnea which occurred while playing outside the home.
On admission, a board certified pediatrician performed auscultation that revealed diminished breath sounds in the left hemithorax. The patient was sent to the radiology department for imaging evaluation.
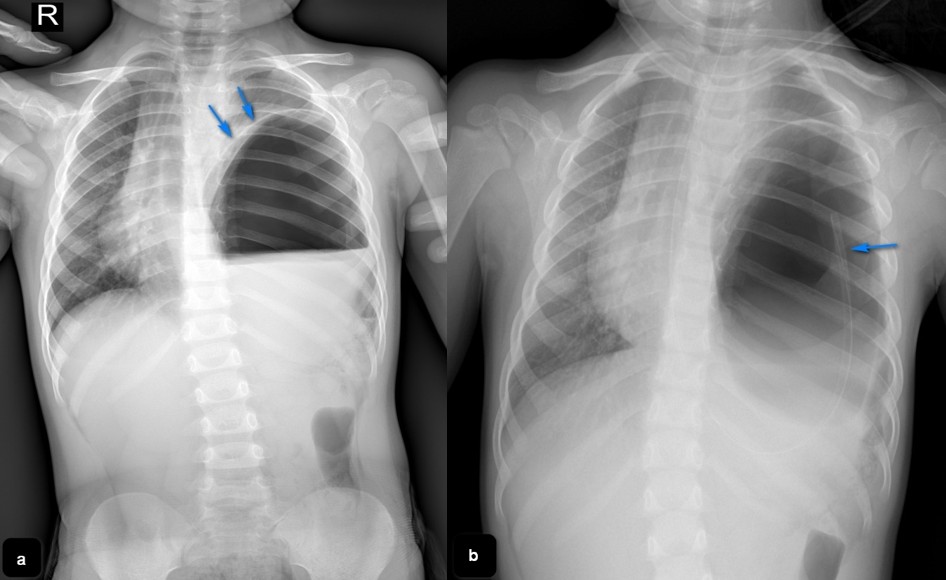
Chest radiography demonstrated an air filled structure with fluid in the left hemithorax and a significant mediastinal shift (Fig. 1a). Initially it was interpreted as hydropneumothorax and the child was admitted to the intensive care unit for thoracocentesis. Gastric gas was not seen in the left upper abdomen after careful observation of the chest X-ray, so the decision was made to insert a nasogastric tube (NGT) which led to the resolution of respiratory symptoms. That directed us to the assumption of potential tension gastrothorax (Fig. 1b). In line with this, the patient was further evaluated by a computerized tomography (CT).
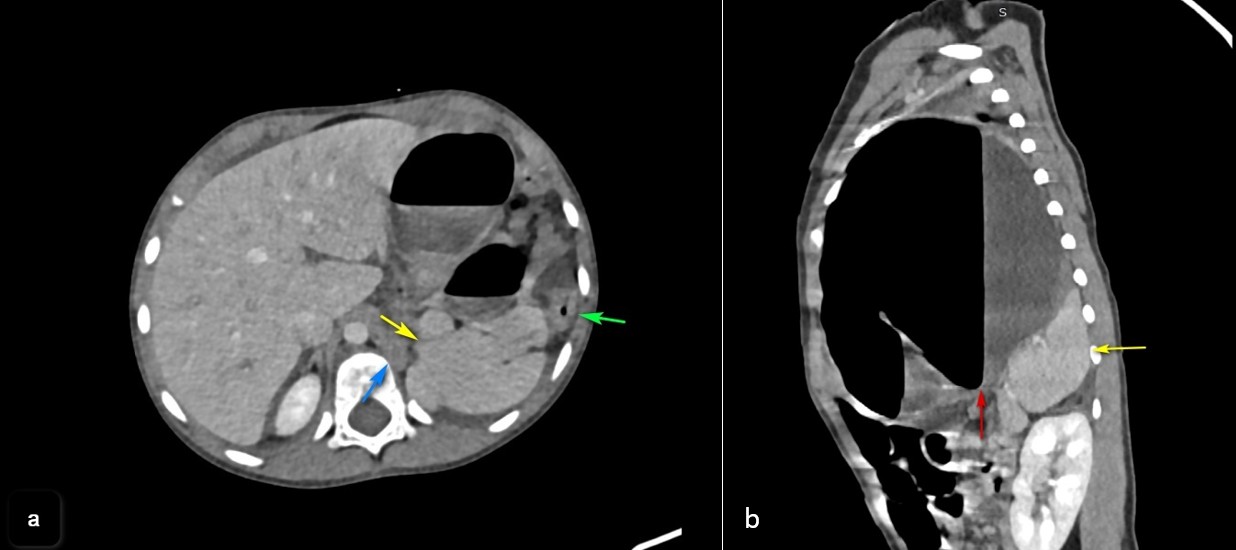
A CT scan was done to confirm the diaphragmatic defect and it revealed stomach in the left hemithorax, filled with air and fluid. The spleen with accessory spleen and left colic flexure had an intrathoracic position. The left lung parenchyma was compressed with signs of right mediastinal shift (Fig. 2a and Fig. 2b).
After the imaging evaluation, the patient was refered to a board sertified pediatric surgeon and underwent surgery the following day. A left subcostal incision was made. Intraoperatively, left posterolateral diaphragmatic defect was verified with multiple organs protruding in the thoracic cavity including the stomach, spleen, part of the colon and great omentum. Organs were repositioned into the abdomen and a reconstruction of the left hemidiaphragm was conducted with direct sutures, thus repairing the existing defect. The operation was performed without complications.
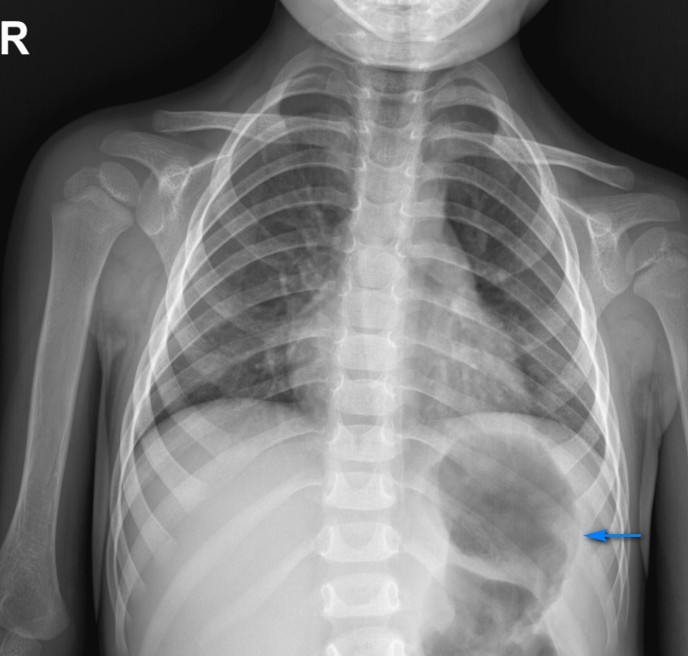
The postoperative course was uneventful and the patient was discharged from the hospital after 7 days (Fig. 3). Follow up exams were performed immediately after surgery and after one week. Since the patient was healthy and without any difficulties he returned to his daily activities. One month after the surgery he showed no complications during the physical exam. No further follow up exams have been performed since.
A written informed consent was obtained from the parents of the patient for this publication.
Discussion
Tension gastrothorax represents intrathoracic position of stomach, distended with air or fluid, causing a mediastinal shift. The most common site of herniation in children is pre-existing left posterolateral diaphragmatic defect (Bochdalek).4 At the level of diaphragmatic defect, increased abdominal pressure causes protrusion of the stomach into the thoracic cavity and twisting of the gastroesophageal junction. This causes a one-way valve mechanism which leads to rapid distension of the stomach with air or fluid.
Initial symptoms can be nonspecific such as abdominal or chest pain, coughing and dyspnea eventually leading to life-threatening conditions such as severe respiratory distress and cardiac arrest.5 Approximately 10% of patients with CDH present after the age of 5 months, with a very small number of those developing tension gastrothorax.6 In the case of severe clinical symptoms in an otherwise healthy child and the need for urgent diagnosis and treatment, mistakes can be made. The presence of an air-filled structure in the left hemithorax with mediastinal shift on the chest X-ray can be misinterpreted as tension pneumothorax.
In the case of tension pneumothorax, the gastric air is seen under the left hemidiaphragm which is well-defined and depressed. The parenchyma of the left lung is medially compressed. On the other hand, the left hemidiaphragm is poorly defined in the case of gastrothorax and a gastric bubble is not seen in the left upper quadrant of the abdomen. Superior margin of the air filled structure is formed by the compressed lung parenchyma and the stomach wall.7
Even though prompt management is needed, careful interpretation of the chest X-ray is essential for the correct diagnosis. In order to confirm the suspicion of tension gastrothorax, an NGT can be placed to show the position of the stomach on the X-ray. The final step in radiological diagnosis is a CT scan of the thorax to precisely visualize all herniated structures.8 Management of tension gastrothorax, when diagnosed, consists of several options. From our experience and upon reviewing the literature, the following are the recommended options:9,10
- Initial treatment should be placing an nasogastric or orogastric tube to decompress the stomach, which may not be easy because of te altered anatomy of esophagogastric junction and can sometimes be done with endoscopic assistance.
- Endoscopic stomach decompression if the patient has stable vital parameters.
- Transthoracic needle decompression of stomach if previous ways of decompression fail or are not possible to be performed due to the patient’s hemodynamic or respiratory worsening, which should be assesed by an anesthesiologist. This method does not have a high success rate and makes a patient susceptible to contamination and infection.
- Emergency laparotomy/thoracotomy, stomach reposition and diaphragmatic defect repair, which is also the definitive treatment in all cases. The laparotomy or thoracotomy approach choice is left for the surgeon to decide. Laparotomy gives the surgeon the option to also explore other organs and provides a more prompt reduction of the stomach while a thoracotomy allows an easier repair of the diaphragm.
This case report aims to add to knowledge of the diagnosis and treatment of tension gastrothorax in pediatric patients.
When the symptoms of respiratory distress occur in a previously healthy child, especially if there was an event leading to increased abdominal pressure, timely and adequate diagnostic methods must be performed to confirm the diagnosis of tension gastrothorax. Prompt management is preceded by an X-ray showing distinct signs opposite to tension pneumothorax. Initial placement of NGT is important for the diagnosis as well as to decompress the stomach, followed by the reduction of the organs into the abdomen and diaphragmatic repair.
Ethical approval
A written informed consent was obtained from the parents of the patient for this publication.
Source of funding
The authors declare the study received no funding.
Conflict of interest
The authors declare that there is no conflict of interest.
References
- Bagłaj M. Late-presenting congenital diaphragmatic hernia in children: a clinical spectrum. Pediatr Surg Int 2004; 20: 658-669. https://doi.org/10.1007/s00383-004-1269-5
- Horst M, Sacher P, Molz G, Willi UV, Meuli M. Tension gastrothorax. J Pediatr Surg 2005; 40: 1500-1504. https://doi.org/10.1016/j.jpedsurg.2005.05.079
- Zedan M, El-Ghazaly M, Fouda A, El-Bayoumi M. Tension gastrothorax: a case report and review of literature. J Pediatr Surg 2008; 43: 740-743. https://doi.org/10.1016/j.jpedsurg.2007.10.072
- Næss PA, Wiborg J, Kjellevold K, Gaarder C. Tension gastrothorax: acute life-threatening manifestation of late onset congenital diaphragmatic hernia (CDH) in children. Scand J Trauma Resusc Emerg Med 2015; 23: 49. https://doi.org/10.1186/s13049-015-0129-8
- Song IH. Tension gastrothorax in late-onset congenital diaphragmatic hernia, a rare but life-threatening condition: a case report. Medicine (Baltimore) 2021; 100: e24815. https://doi.org/10.1097/MD.0000000000024815
- Coren ME, Rosenthal M, Bush A. Congenital diaphragmatic hernia misdiagnosed as tension pneumothorax. Pediatr Pulmonol 1997; 24: 119-121. https://doi.org/cmfbrn
- Muzzafar S, Swischuk LE, Jadhav SP. Radiographic findings in late-presenting congenital diaphragmatic hernia: helpful imaging findings. Pediatr Radiol 2012; 42: 337-342. https://doi.org/10.1007/s00247-011-2226-9
- Rashid F, Chakrabarty MM, Singh R, Iftikhar SY. A review on delayed presentation of diaphragmatic rupture. World J Emerg Surg 2009; 4: 32. https://doi.org/10.1186/1749-7922-4-32
- Ng J, Rex D, Sudhakaran N, Okoye B, Mukhtar Z. Tension gastrothorax in children: introducing a management algorithm. J Pediatr Surg 2013; 48: 1613-1617. https://doi.org/10.1016/j.jpedsurg.2013.05.066
- Bunya N, Sawamoto K, Uemura S, et al. How to manage tension gastrothorax: a case report of tension gastrothorax with multiple trauma due to traumatic diaphragmatic rupture. Int J Emerg Med 2017; 10: 4. https://doi.org/10.1186/s12245-017-0131-1
Copyright and license
Copyright © 2025 The Author(s). This is an open access article distributed under the Creative Commons Attribution License (CC BY), which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is properly cited.