Graphical Abstract
Abstract
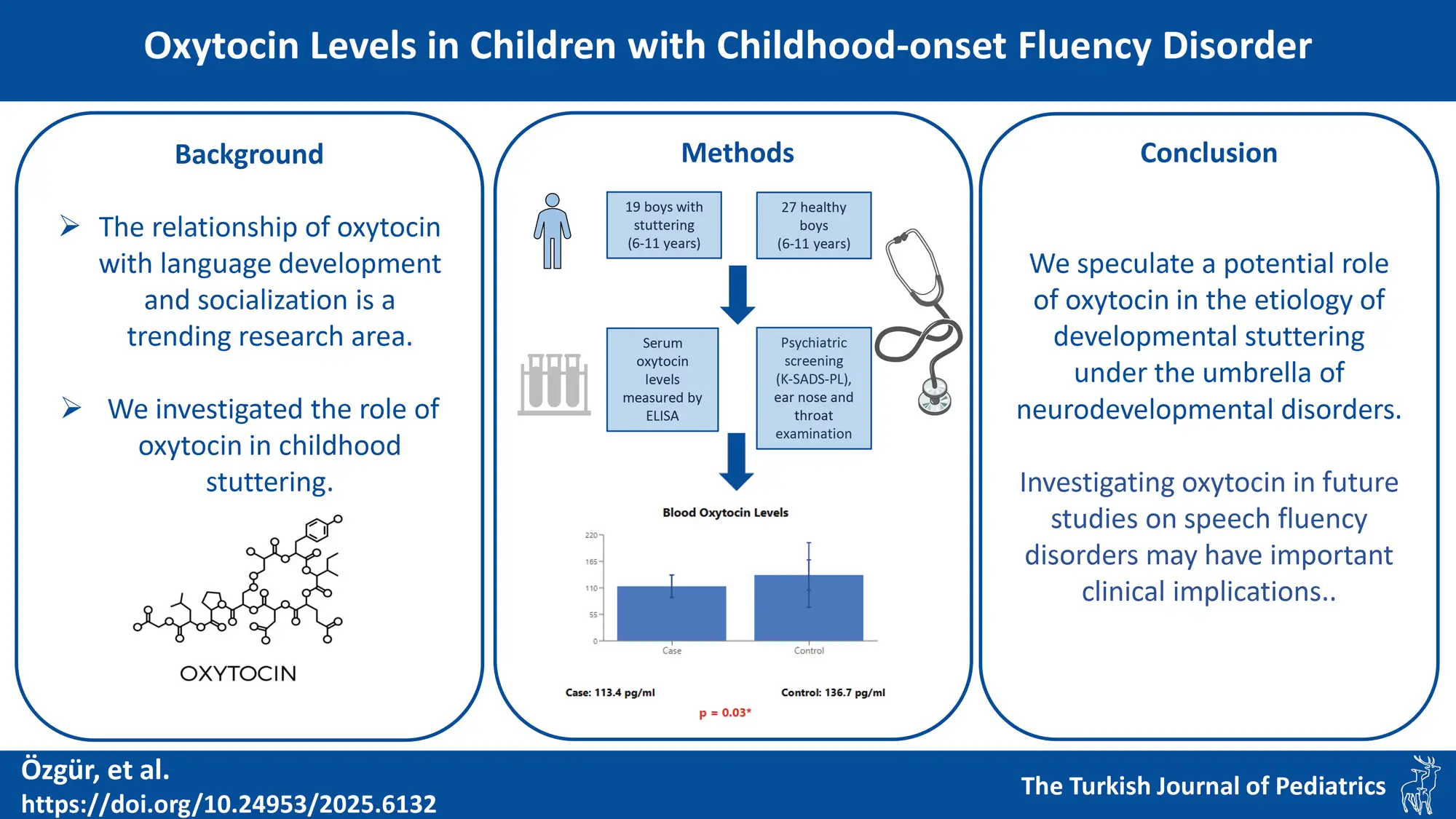
Background. Evidence suggests a role for oxytocin in language development and cognitive functions in humans. However, there is a lack of research investigating the role of oxytocin in childhood-onset fluency disorder (stuttering). The aim of this study is to compare blood oxytocin levels between children diagnosed with stuttering and healthy controls.
Methods. Nineteen male children diagnosed with stuttering, aged between 6 and 11 years, and 27 typically fluent male children as a control group were included. All participants underwent psychiatric screening using the semi-structured interview The Kiddie Schedule for Affective Disorders and Schizophrenia School-Age Children-Present and Lifetime Version, and an ear, nose, throat examination. Serum oxytocin levels were determined using enzyme-linked immunosorbent assay.
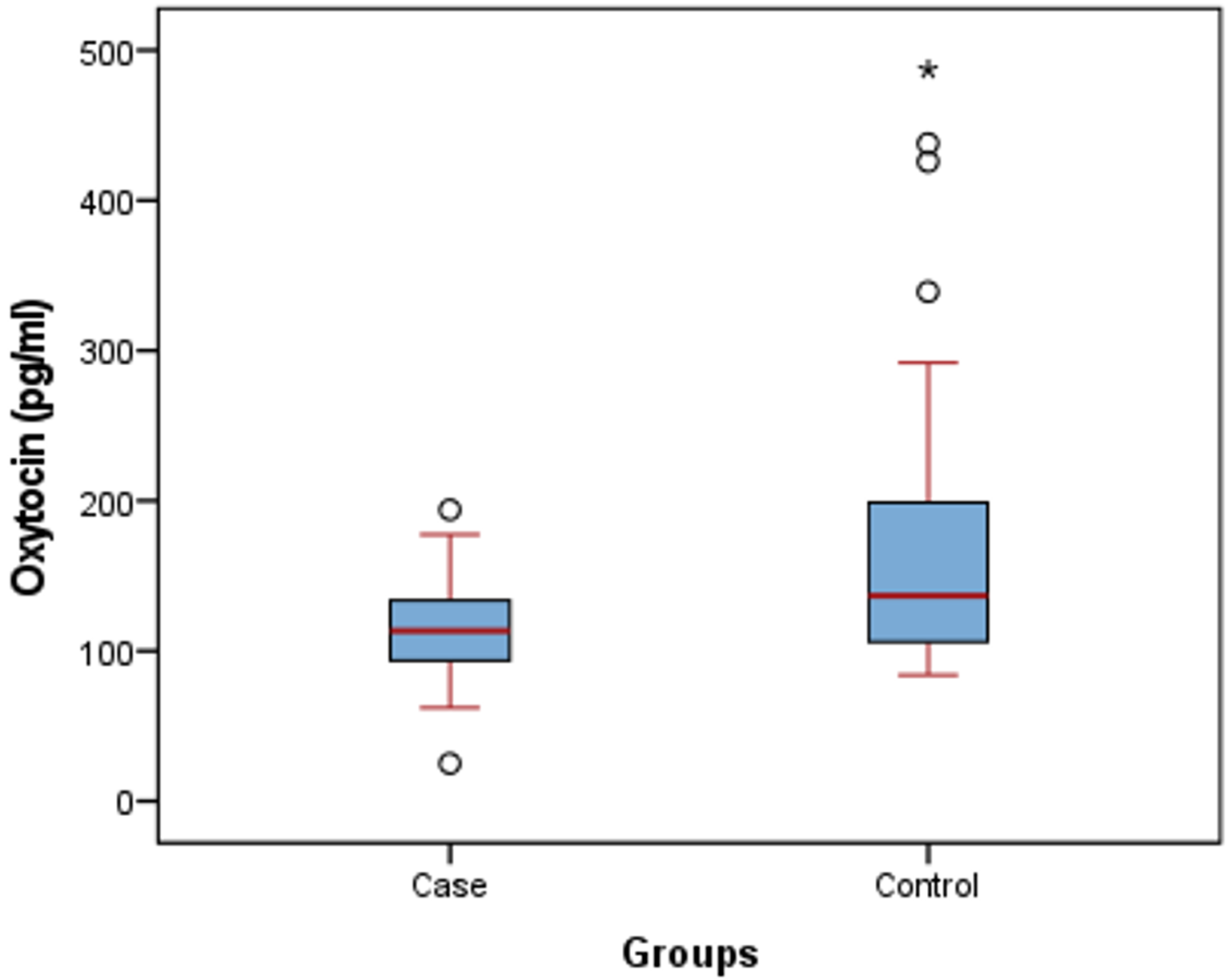
Results. The median (Q1-Q3) blood oxytocin levels in the case group were 113.4 (90.19-136.3) pg/mL, while in the control group were 136.7 (105.4-203.7) pg/mL. A statistically significant lower level of oxytocin was observed in the case group compared to the control group (U=162, p=0.03).
Conclusions. We speculate a potential role of oxytocin in the etiology of developmental stuttering under the umbrella of neurodevelopmental disorders. The investigation of oxytocin, which plays a role in socialization and speech, in future studies on speech fluency disorders is intriguing in terms of its implications for clinical applications, including treatment.
Keywords: stuttering, childhood, oxytocin, speech disorders, fluency disorder
Introduction
Childhood-onset fluency disorder, commonly referred to as stuttering, is a communication disorder marked by disruptions in the natural flow and timing of speech that are not typical for a person’s age. These findings and symptoms are included among the diagnostic criteria for “childhood onset fluency disorder”, which falls under the communication disorders classification within the category of neurodevelopmental disorders in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5).1 Approximately 80%-90% of all developmental stuttering cases begin before the age of 6.1 Childhood stuttering is a multifactorial diagnosis involving genetic, psychological, neurological, and behavioral characteristics. In treatment, focus should be placed on each contributing factor.2-5 Among the neurogenic factors implicated in etiology are differences in the gray-white matter ratio of the brain, variations in neuronal network connections, atypical lateralization of hemisphere functions, and increased white matter connections in the right hemisphere.6-8
Oxytocin, a neurohypophyseal peptide, is secreted from the paraventricular and supraoptic nuclei and is primarily associated with uterine contractions during childbirth and milk ejection during lactation. In both men and women, oxytocin is believed to play a role in sexual and maternal behavior, social recognition, aggression, cognition, and neuromodulation through its central and peripheral effects.9,10 It is believed that the activation of oxytocin receptors may play an important role in developmental processes and cell differentiation. The presence of oxytocin receptors in various brain regions supports this view. Some studies in both animals and humans have demonstrated the role of oxytocin in social communication, auditory processing, and speech behavior.11,12 A recent study by Theofanopoulou suggests that oxytocin may play a role in language development and cognitive functions in humans.13 Another piece of evidence supporting the effects of oxytocin on speech is the finding that oxytocin receptors are more abundant in the left hemisphere, where speech and auditory centers are located, compared to the right hemisphere.14 All of these findings support the hypothesis that oxytocin plays a role in social relationships, auditory and speech behavior development in mammals.
Previous studies have reported the role of oxytocin in speech development. Considering studies suggesting the role of oxytocin in neurodegenerative and neurodevelopmental disorders15, we decided to examine oxytocin levels in speech disorders, which are classified as neurodevelopmental disorders. A literature review did not reveal any study investigating the role of oxytocin in the etiology of speech fluency disorders in children. Our hypothesis posits that blood oxytocin levels in children with speech fluency disorders will be lower compared to healthy controls.
Materials and Methods
Ethics and consent
The study obtained ethical approval from the Muğla Sıtkı Koçman University Clinical Research Ethics Committee. The study was conducted in accordance with the principles of the Declaration of Helsinki. Written informed consent forms were obtained from the children and their parents for participation in the study.
Participants
Between January 2020 and July 2020, children presenting with complaints of impaired speech fluency, frequent repetitions, or prolongations of sounds or syllables at the Child and Adolescent Psychiatry and/or Ear, Nose, and Throat (ENT) outpatient clinics of Muğla Education and Research Hospital, and diagnosed with stuttering, were consecutively enrolled as the case group (n=28). To eliminate the potential influence of sex and age on oxytocin levels, only male participants in the prepubertal age group (6-11 years old) were included in the study. Age and sex matched typically fluent children without a psychiatric diagnosis upon psychiatric examination and with normal ENT examination, who presented to the ENT outpatient clinic for reasons other than communication problems (e.g. preoperative evaluation), were included as the control group.
Procedures
Childhood-onset fluency disorder (stuttering) was diagnosed by using the DSM-5 criteria during psychiatric examination.1 All participants were administered the Kiddie Schedule for Affective Disorders and Schizophrenia School-Age Children-Present and Lifetime Version-(K-SADS-PL) by a child and adolescent psychiatrist to exclude psychiatric diagnoses. Children with non-fluency communication disorders, additional psychiatric diagnoses, neurological disorders, physical conditions such as cleft palate-lip that may contribute to speech disorder, and those clinically diagnosed with intellectual disability were excluded from the study. Additionally, all children presenting with stuttering underwent otolaryngological examination and hearing assessment by an ENT specialist. A socio-demographic data form prepared by the researchers was administered. This form included information such as the participants’ and parents’ age, education level, occupation, marital status, medical history, number of siblings, presence of motor movements accompanying stuttering, family history, onset time of stuttering, and whether the participant received treatment for stuttering.
Psychiatric assessment tools
The Kiddie Schedule for Affective Disorders and Schizophrenia School-Age Children-Present and Lifetime Version-Present And Life Time Version (K-SADS-PL) DSM-5: K-SADS-PL, the semi-structured interview form used in this study, is designed to inquire about psychiatric diagnoses in children and adolescents aged 6-18 years in accordance with the DSM-5 diagnostic criteria.16 A detailed psychiatric assessment is conducted with both parents and children face-to-face. The Turkish validity and reliability of this assessment have been established by Ünal et al.17 In the case group, 9 cases were excluded due to comorbid psychiatric diagnoses.
Measurement of serum oxytocin concentrations
Fasting venous blood samples were collected from participants into gel-separated blood tubes by venipuncture (between 8-10 a.m.). The blood tubes were centrifuged at 2000 g for 10 minutes and stored at -80 °C until analysis of oxytocin levels.
Serum oxytocin concentrations were measured by a human oxytocin enzyme-linked immunosorbent assay (ELISA) kit (Cat# E1046Hu, Bioassay Technology Laboratory, Shanghai, China) according to the instructions given in the package insert. The sensitivity of the oxytocin assay was 1.06 pg/mL. Inter-assay and intra-assay coefficients of variation of assay were < 10%. The measuring range for assay was 2 to 600 pg/mL.
Data analysis
The data were analyzed using SPSS 29.0 (IBM Corp., USA). Descriptive statistics were reported using frequency, percentage, mean, standard deviation, and median (25th-75th percentile, Q1-Q3). The normal distribution of the data was assessed using the Kolmogorov-Smirnov test. Chi square test was used to compare categorical variables. Mann Whitney U test, one of the nonparametric tests, was used to compare two independent groups that were not normally distributed. A p-value less than 0.05 was considered statistically significant.
Results
The study comprised 45 boys aged 6–11 years, including 19 diagnosed with stuttering (case group) and 27 typically fluent peers (control group). The median age of the case group was 9 (7-10) years, and 8 (7-10) years in the control group with no statistically significant difference in age between the groups (p=0.751). Among those diagnosed with stuttering, 8 (42.1%) had involuntary motor movements accompanying stuttering (e.g. jerking of the head, eye blinks, stomping the foot) and 12 (63.2%) had a family history of stuttering. The mean age of onset of stuttering symptoms was 5.05 ± 1.7 years. There was no statistically significant difference in sociodemographic characteristics such as grade level, age of parents, parental education level, employment status, and marital status between the case and control groups (Table I).
|
N/A: not applicable * Mann-Whitney U test, ** Chi square test. |
|||
| Table I. Sociodemographic characteristics of stuttering and control groups | |||
|
|
|
|
|
| Age, yr, median (Q1-Q3) |
|
|
|
| School, n (%) |
|
||
| Pre-school |
|
|
|
| Primary school |
|
|
|
| Secondary school |
|
|
|
| Mother’s age, yr, median (Q1-Q3) |
|
|
|
| Father’s age, yr, median (Q1-Q3) |
|
|
|
| Maternal employment, n (%) |
|
|
|
| Paternal employment, n (%) |
|
|
|
| Mother's education level, n (%) |
|
||
| Less than high school |
|
|
|
| High school graduate |
|
|
|
| University graduate |
|
|
|
| Father's education level, n (%) |
|
||
| Less than high school |
|
|
|
| High school graduate |
|
|
|
| University graduate |
|
|
|
| Parental consanguinity, n (%) |
|
|
|
| Parents currently married, n (%) |
|
|
|
| Chronic disease in the child, n (%) |
|
|
|
| Family history of stuttering, n (%) |
|
|
|
| Speech language therapy, n (%) |
|
|
|
| Accompanying motor movement, n (%) |
|
|
|
The median blood oxytocin levels were 113.4 (90.19-136.3) pg/mL in the case group, and 136.7 (105.4-203.7) pg/mL in the control group (Fig. 1). Upon comparing the blood oxytocin levels between the groups, oxytocin levels in the case group were statistically significantly lower (U=162, p=0.03). There was no significant difference in blood oxytocin levels based on the presence or absence of involuntary motor movements accompanying stuttering in the case group (U=38, p=0.62).
Discussion
There are limited studies on the role of oxytocin in speech disorders, but scientific evidence supports its effects on communication and speech. This study aims to investigate the relationship between oxytocin and stuttering, a speech disorder.
The results obtained from the study revealed that blood oxytocin levels in children with stuttering were significantly lower. This finding can be considered as an important clue suggesting the potential role of oxytocin neurohormone in the etiology of stuttering. Since there are no studies investigating blood oxytocin levels in individuals with stuttering in the literature, the results could not be compared. However, there are studies on certain hormones that may be associated with stuttering. Selcuk et al. reported that testosterone levels were higher in children with stuttering compared to the control group.18 Researchers have suggested that high levels of sex hormones may increase stress in individuals, and it is proposed that high stress levels may trigger stuttering. In addition to serum testosterone levels, some studies have investigated the 2nd digit to 4th digit ratio (2D:4D) as an indicator of prenatal testosterone levels, and differences in prenatal testosterone levels have been reported to be associated with stuttering.19,20 Mohammadi et al. reported that serum testosterone, dihydrotestosterone, and estradiol levels were significantly higher in the stuttering group.21 The investigation of sex hormones in stuttering stems from the fact that stuttering is more prevalent in males.
In our study, we included patients of the same developmental period and male sex to exclude age and sex factors that could affect blood hormone levels. Although oxytocin is not a sex hormone, studies in adults have reported that blood oxytocin levels vary according to sex and age periods.22,23 There is a need for studies investigating changes in oxytocin levels in children according to age periods.
The relationship between oxytocin and psychosocial behaviors, as well as its role in the etiology of certain psychiatric disorders, is intriguing. The discovery of oxytocin receptors being more densely populated in certain areas of the brain, particularly those associated with speech and hearing in the left hemisphere compared to the right hemisphere, as reported by Mitre et al., can be considered as a significant finding supporting the effects of oxytocin on speech.14
A recent study investigating the effects of intranasal oxytocin administration and the oxytocin receptor (rs53576) on speech using functional magnetic resonance imaging demonstrated that oxytocin increased brain activity in sensorimotor cortices, both dorsal and right ventral speech processing streams, as well as subcortical and cortical limbic and executive control regions. It was also shown that in some of these regions, the rs53576 OXTR polymorphism modulated brain activity associated with oxytocin administration.24 Studies on the role of oxytocin in both normal speech and speech disorders will help elucidate its neuroimaging, neurophysiological, and biochemical effects.
In this study, anxiety disorders were also excluded from the study to eliminate the influence of additional psychopathologies on oxytocin levels. Oxytocin suppresses activity in amygdala neurons associated with other brain regions related to fear, such as the anterior cingulate cortex (ACC) and the medial prefrontal cortex (MPC).25,26 It was discovered that oxytocin diminishes heightened activation of the ACC and MPC in individuals experiencing social anxiety disorder when exposed to sad faces.26 The absence of a diagnosis of social anxiety disorder or other anxiety disorders in children of the age range studied in this research does not necessarily mean they won’t develop them later in life. Additionally, which stuttering children will develop anxiety disorders remains a topic that requires further research. Whether current oxytocin levels serve as a biomarker for anxiety disorders in stuttering children is also an intriguing topic for future studies.
The lack of examination into the relationship between stuttering severity and oxytocin and failure to compare oxytocin levels across different age groups (under 6 years old, over 11 years old) are limitations of this study. Another limitation is that the study was completed with a small sample size due to a decrease in the number of cases presenting to the clinic during the coronavirus disease 2019 pandemic. Restricting the age range to prepubertal and including only males can be considered the strengths of the study.
Conclusion
This study is pioneering in its examination of oxytocin levels in stuttering. However, the role of oxytocin in the onset of speech disorders cannot be conclusively determined based on the observed differences in oxytocin levels alone.
In light of all this information, we believe that oxytocin may play a potential role in the etiology of developmental stuttering, which falls under the umbrella of neurodevelopmental disorders. Further studies examining oxytocin levels in speech disorders will help determine the reproducibility of our results. Additionally, research investigating the role of oxytocin in socialization and speech will shed light on its place in the etiology of speech fluency disorders, thus expanding treatment options in the literature.
Ethical approval
The study was approved by Muğla Sıtkı Koçman University Clinical Research Ethics Committee (date: 16.01.2020, number: 01/VIII).
Source of funding
The authors declare the study received no funding.
Conflict of interest
The authors declare that there is no conflict of interest.
References
- American Psychiatric Association, DSM-5 Task Force. Diagnostic and statistical manual of mental disorders: DSM-5. 5th ed. Washington, DC: American Psychiatric Association; 2013: xliv, 947. https://doi.org/10.1176/appi.books.9780890425596
- Smith A, Weber C. How stuttering develops: the multifactorial dynamic pathways theory. J Speech Lang Hear Res 2017; 60: 2483-2505. https://doi.org/10.1044/2017_JSLHR-S-16-0343
- Packman A. Theory and therapy in stuttering: a complex relationship. J Fluency Disord 2012; 37: 225-233. https://doi.org/10.1016/j.jfludis.2012.05.004
- Starkweather CW, Givens-Ackerman J. Stuttering. Austin, TX: Pro-Ed; 1997.
- Smith A, Kelly E. Stuttering: a dynamic, multifactorial model. In: Curlee RF, Siegel GM, editors. Nature and treatment of stuttering: new directions. 2nd ed. Boston, MA: Allyn & Bacon; 1997: 204-217.
- Chang SE, Erickson KI, Ambrose NG, Hasegawa-Johnson MA, Ludlow CL. Brain anatomy differences in childhood stuttering. Neuroimage 2008; 39: 1333-1344. https://doi.org/10.1016/j.neuroimage.2007.09.067
- Chang SE, Zhu DC. Neural network connectivity differences in children who stutter. Brain 2013; 136: 3709-3726. https://doi.org/10.1093/brain/awt275
- Song LP, Peng DL, Jin Z, et al. Gray matter abnormalities in developmental stuttering determined with voxel-based morphometry. Zhonghua Yi Xue Za Zhi 2007; 87: 2884-2888.
- Greenamyre JT, Betarbet R, Sherer TB. The rotenone model of Parkinson’s disease: genes, environment and mitochondria. Parkinsonism Relat Disord 2003; 9(Suppl. 2): S59-S64. https://doi.org/10.1016/s1353-8020(03)00023-3
- Gutkowska J, Jankowski M. Oxytocin: old hormone, new drug. Pharmaceuticals (Basel) 2009; 2: 168-183. https://doi.org/10.3390/ph203168
- Boccia ML, Petrusz P, Suzuki K, Marson L, Pedersen CA. Immunohistochemical localization of oxytocin receptors in human brain. Neuroscience 2013; 253: 155-164. https://doi.org/10.1016/j.neuroscience.2013.08.048
- Clark-Elford R, Nathan PJ, Auyeung B, et al. The effects of oxytocin on social reward learning in humans. Int J Neuropsychopharmacol 2014; 17: 199-209. https://doi.org/10.1017/S1461145713001120
- Theofanopoulou C. Implications of oxytocin in human linguistic cognition: from genome to phenome. Front Neurosci 2016; 10: 271. https://doi.org/10.3389/fnins.2016.00271
- Mitre M, Marlin BJ, Schiavo JK, et al. A distributed network for social cognition enriched for oxytocin receptors. J Neurosci 2016; 36: 2517-2535. https://doi.org/10.1523/JNEUROSCI.2409-15.2016
- Ghazy AA, Soliman OA, Elbahnasi AI, Alawy AY, Mansour AM, Gowayed MA. Role of oxytocin in different neuropsychiatric, neurodegenerative, and neurodevelopmental disorders. Rev Physiol Biochem Pharmacol 2023; 186: 95-134. https://doi.org/10.1007/112_2022_72
- Kaufman J, Birmaher B, Axelson D, Perepletchikova F, Brent D, Ryan N. Schedule for affective disorders and schizophrenia for school-aged children: present and life time version (K-SADS-PL) DSM-5 November 2016 working draft. New Haven: Yale University, Child and Adolescent Research and Education; 2016.
- Ünal F, Öktem F, Çetin-Çuhadaroğlu F, et al. Reliability and validity of the schedule for affective disorders and schizophrenia for school-age children-present and lifetime version, DSM-5 November 2016-Turkish Adaptation (K-SADS-PL-DSM-5-T). Türk Psikiyatri Dergisi 2019; 30: 42-50. https://doi.org/10.5080/u23408
- Selçuk EB, Erbay LG, Özcan ÖÖ, Kartalci Ş, Batcioğlu K. Testosterone levels of children with a diagnosis of developmental stuttering. Ther Clin Risk Manag 2015; 11: 793-798. https://doi.org/10.2147/TCRM.S83129
- Montag C, Bleek B, Breuer S, et al. Prenatal testosterone and stuttering. Early Hum Dev 2015; 91: 43-46. https://doi.org/10.1016/j.earlhumdev.2014.11.003
- Dönmez YE, Özcan Ö, Bilgiç A, Miniksar DY. The relationship between prenatal testosterone and developmental stuttering in boys. Turk J Pediatr 2019; 61: 193-199. https://doi.org/10.24953/turkjped.2019.02.007
- Mohammadi H, Joghataei MT, Rahimi Z, et al. Sex steroid hormones and sex hormone binding globulin levels, CYP17 MSP AI (-34T:C) and CYP19 codon 39 (Trp:Arg) variants in children with developmental stuttering. Brain Lang 2017; 175: 47-56. https://doi.org/10.1016/j.bandl.2017.09.004
- Marazziti D, Baroni S, Mucci F, et al. Sex-related differences in plasma oxytocin levels in humans. Clin Pract Epidemiol Ment Health 2019; 15: 58-63. https://doi.org/10.2174/1745017901915010058
- Zak PJ, Curry B, Owen T, Barraza JA. Oxytocin release increases with age and is associated with life satisfaction and prosocial behaviors. Front Behav Neurosci 2022; 16: 846234. https://doi.org/10.3389/fnbeh.2022.846234
- Vogt C, Floegel M, Kasper J, Gispert-Sánchez S, Kell CA. Oxytocinergic modulation of speech production-a double-blind placebo-controlled fMRI study. Soc Cogn Affect Neurosci 2023; 18: nsad035. https://doi.org/10.1093/scan/nsad035
- Huber D, Veinante P, Stoop R. Vasopressin and oxytocin excite distinct neuronal populations in the central amygdala. Science 2005; 308: 245-248. https://doi.org/10.1126/science.1105636
- Labuschagne I, Phan KL, Wood A, et al. Medial frontal hyperactivity to sad faces in generalized social anxiety disorder and modulation by oxytocin. Int J Neuropsychopharmacol 2012; 15: 883-896. https://doi.org/10.1017/S1461145711001489
Copyright and license
Copyright © 2025 The Author(s). This is an open access article distributed under the Creative Commons Attribution License (CC BY), which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is properly cited.