Graphical Abstract
Abstract
Introduction. Blunt impact-induced traumatic abdominal wall hernia (TAWH) is classically associated with handlebar injury caused by direct trauma to the anterior abdominal wall, hence the term “handlebar hernia.” It is uncommon in children and associated with significant morbidity if diagnosis is delayed.
The aim of this study is to present our experience in treating bicycle handlebar-associated TAWH, highlight the likelihood of associated intra-abdominal injuries, and emphasize the importance of early imaging and surgical intervention when necessary.
Case Presentation. Three cases of abdominal wall hernia were included. All patients were boys, with a mean age of 8.6 years (range: 7–11 years). All patients presented with swelling in the iliac fossa (right n= 2 and left n= 1). Emergency computed tomography (CT) was performed in all cases: two revealed a muscular defect, while the third showed pneumoperitoneum. The musculoaponeurotic defect was surgically repaired in each case. In the third patient, a small intestinal perforation was also identified and sutured. All patients recovered uneventfully.
Conclusion. TAWH is a rare clinical entity that may signal more significant associated injuries, such as hollow viscus perforation, which often requires urgent surgery. A high index of suspicion is necessary in children presenting with bruising, abrasions, ecchymosis, hematoma, or peritoneal signs following blunt abdominal trauma, and there should be a low threshold for additional imaging.
Keywords: abdominal injuries, child, hernia, trauma
Introduction
Traumatic abdominal wall hernia (TAWH) typically results from blunt trauma to the abdominal wall, leading to disruption of the muscular and fascial layers while the skin remains intact. This injury allows intra-abdominal contents, such as the small bowel, to protrude through the defect.1 The incidence of TAWH is estimated at up to 9% of abdominal wall defects caused by trauma.2 The first case of TAWH described in the literature occurred in 1906, in an adult injured by a wheelbarrow handle.3 Pediatric TAWH was first reported in 1956, in a 14-year-old boy struck in the abdomen by motorcycle handlebars.4 These injuries are difficult to diagnose clinically and lack standardized treatment strategies. Repair usually involves surgical exploration and layered closure of the defect, depending on its size, location, and the condition of surrounding tissues.5 Reporting rare and distinctive presentations, such as traumatic hernia without skin penetration, enriches the literature and helps guide optimal management. In this article, we present three pediatric cases of handlebar-associated abdominal wall hernia.
Case Presentations
Case 1
A 7-year-old boy with no relevant medical history presented to the pediatric surgery emergency department after falling from his bicycle. On examination, a 3-cm swelling with bruising was observed in the right iliac fossa (RIF), extending to the right inguinal region (Fig. 1). Manual palpation revealed tenderness in the lower abdomen. The patient’s pulse was 94 bpm, and his blood pressure was 110/60 mmHg.

An emergency abdominal computed tomography (CT) scan revealed a 30-mm muscular defect in the external oblique muscle, with no associated intestinal perforation.
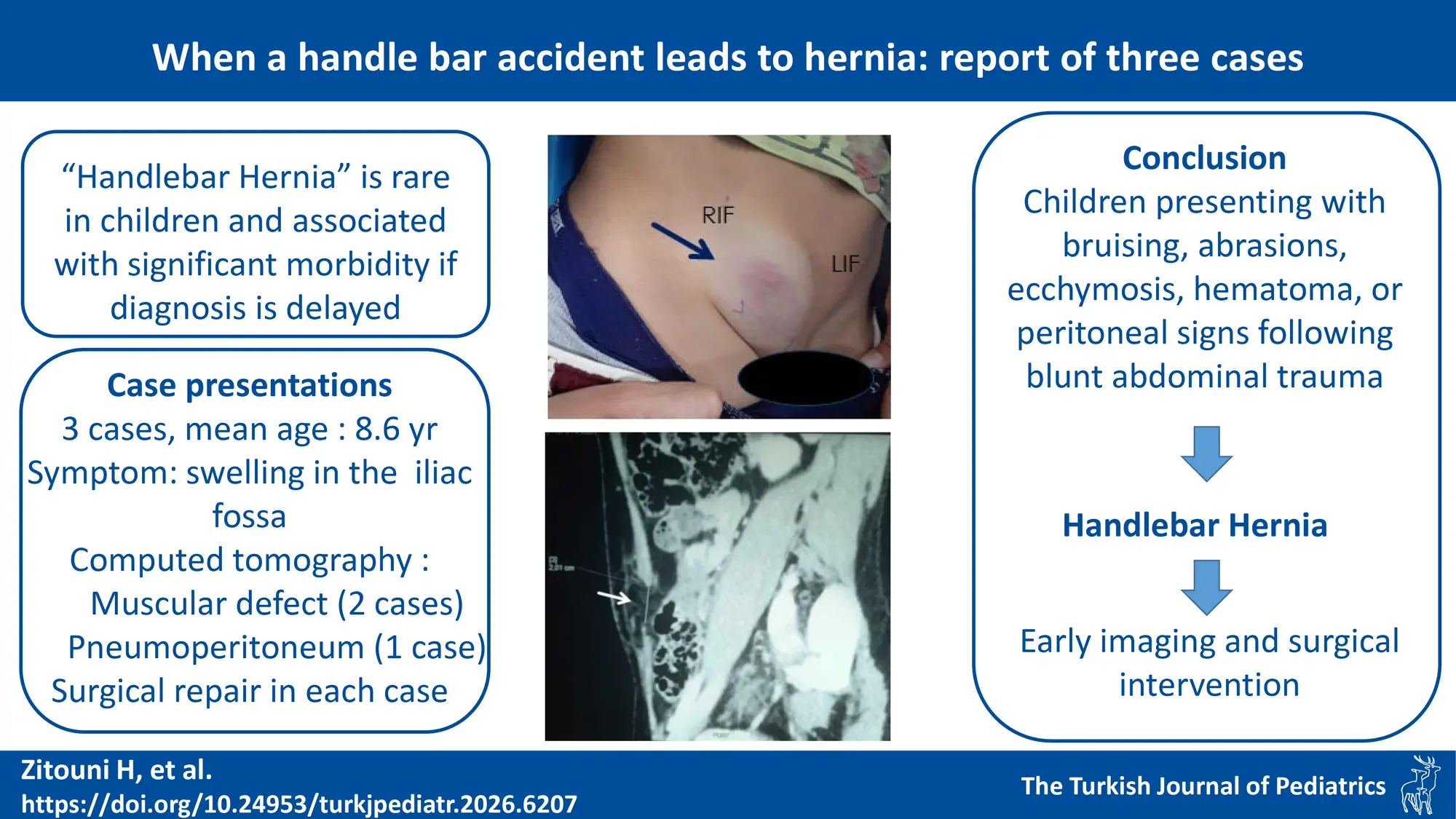
Emergency surgery was performed, during which a 2-cm musculoaponeurotic defect was identified (Fig. 2). The abdominal wall was repaired in layers using interrupted sutures. The postoperative course was uneventful. At 3 months postoperatively, the patient had a strong and intact abdominal wall.
Case 2
An 11-year-old boy with no relevant medical history presented with blunt abdominal trauma caused by impact from a bicycle handlebar to the RIF. Examination revealed a painful 5-cm swelling in the RIF with a 2-cm contusion. The rest of the abdomen was soft, compressible, and non-tender. The patient was hemodynamically stable.
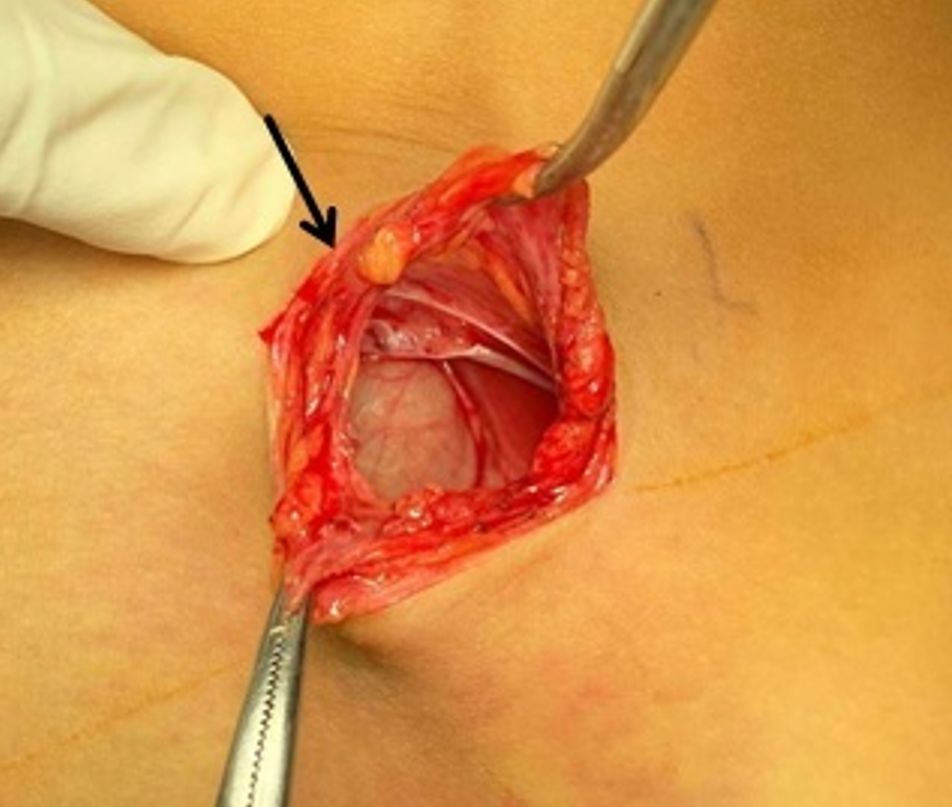
An abdominal CT scan showed a 20-mm defect in the right anterolateral abdominal wall with herniation of subcutaneous epiploic fat (Fig. 3). No other injuries were noted.
An urgent laparotomy was performed through local wound exploration. A 2-cm parietal defect was identified without digestive perforation. The abdominal wall was repaired in layers. Postoperative recovery was uneventful.
Case 3
An 8-year-old boy was referred for abdominal pain following a fall from a bicycle. The child had no relevant medical history, including no history of abdominal hernias. He presented with abdominal pain, vomiting, and bowel dysfunction. Physical examination revealed a tender lump in the left iliac fossa. No additional symptoms were reported. Vital signs were within normal limits.
An abdominal CT scan demonstrated intestinal loops protruding through a 30-mm defect in the abdominal wall, along with significant pneumoperitoneum and subcutaneous emphysema—findings consistent with a perforated hollow viscus.
An emergency laparotomy was performed following a diagnostic laparoscopy. A 3-cm defect in the abdominal wall, a perforation in a viable segment of the small bowel, and a tear in the mesentery of the mid-jejunum were found (Fig. 4). The procedure included a primary wedge resection and closure of the enterotomy, repair of the mesenteric tear, and layered closure of the abdominal wall hernia. The postoperative course was uneventful.

Written informed consent for the publication of the patients’ clinical data and images was obtained from their parents.
Discussion
TAWH is a rare pediatric condition, mostly recorded in case reports, with anatomical abnormalities that vary from minor muscular tears to significant aponeurotic and skeletal damage.6 These injuries often originate from a rapid, localized application of severe blunt force to the abdomen, such as from a bicycle handlebar. This impact causes tangential shearing forces and abrupt increases in intra-abdominal pressure, which disrupts deeper muscle and fascial tissues while the very elastic overlying skin often remains intact.7,8
Due to the great variety in presentation, even expert pediatricians or surgeons may overlook minor injuries, especially when confounding symptoms are present. However, several factors should raise suspicion of TAWH, such as a history of abdominal trauma or a pre-existing hernia. TAWH commonly affects school-aged children and often presents with non-specific symptoms like fever, vomiting, or abdominal pain. Physical examination may reveal bruising, ecchymosis, swelling, or a tender mass—though skin defects are often absent.9-11
Bicycle handlebar trauma should always raise suspicion, even if external signs seem trivial. Studies have shown that physical examination has low sensitivity for detecting TAWH, with rates between 29.4% and 42.3%.12,13 Vu and Klinkner reported that patients with severe handlebar injuries often had only a minor fall at low speeds, with minimal external evidence of trauma.14
TAWH is rarely isolated and is frequently accompanied by associated intra-abdominal injuries, occurring in 25%-79% of cases—as seen in our third case.15,16 The risk of intra-abdominal injuries increases significantly when the handlebar impact occurs in the upper abdomen.
Given the limitations of physical examination in diagnosing TAWH, paraclinical investigations are essential. Although ultrasonography can sometimes detect a TAWH, CT remains the most reliable diagnostic modality.17
According to Burt et al.13, CT imaging has a sensitivity of 98% for identifying traumatic abdominal wall hernias. In addition to visualizing the hernia itself, CT scans can reveal other surgically significant injuries, such as bowel perforations or hemoperitoneum, and can clearly delineate muscular disruptions, which may otherwise be misinterpreted as hematomas or remain undetected altogether.18 It is believed that pain and muscle spasms can obscure these defects on initial imaging, leading to delayed diagnosis.19 In our cases, the clinical presentations were typically marked, and diagnosis was confirmed via CT imaging.
The most severe form of abdominal wall injury, characterized by evisceration, occurs in fewer than 1.5% of blunt abdominal trauma patients.14 In non-operative settings, emergency physicians may attempt gentle reduction of eviscerated bowel loops without applying force. If unsuccessful, the herniated contents should be covered with sterile, non-adhesive, water-impermeable material, and broad-spectrum antibiotics should be initiated immediately.20
Immediate surgical exploration and repair are generally recommended to prevent early complications from unrecognized intra-abdominal injuries, and late complications such as incarceration, strangulation, or bowel ischemia.21
Some authors recommend early repair via a midline incision for anterior TAWHs, particularly in patients already undergoing laparotomy. In contrast, elective repair may be considered for isolated lumbar or lateral TAWHs. Primary closure of all abdominal wall layers is the standard approach. While prosthetic mesh is often used in adults for larger defects, in children, the vast majority of TAWHs in children can be repaired primarily without mesh.22,23
If the overlying skin shows signs of trauma (e.g., abrasions or hematomas), elective surgery is often postponed until soft-tissue recovery to minimize the risk of wound dehiscence and further tissue damage.24
Although laparotomy is the most commonly used surgical approach in the literature (approximately 85%), laparoscopy has emerged as a valuable alternative. Minimally invasive techniques can help exclude intra-abdominal injuries and may eliminate the need for a midline laparotomy, particularly in hemodynamically stable patients—as illustrated by our third case.10
In carefully selected cases with no associated intra-abdominal injuries, conservative management may be considered. However, this requires close clinical and radiological monitoring, and current evidence does not support routine non-operative management of TAWH.25,26
Conclusion
Traumatic abdominal wall hernia caused by bicycle handlebar injuries in children is a rare but important clinical entity. Early recognition and intervention are crucial to prevent morbidity associated with bowel strangulation and incarceration.
Clinicians should maintain a high index of suspicion for TAWH in any child presenting with abdominal trauma from handlebars—especially when accompanied by the “handlebar sign” (localized bruising or swelling). A low threshold for imaging, particularly with CT scanning, is essential.
Surgical repair, whether open or laparoscopic, remains the cornerstone of management. While non-surgical approaches have been reported in isolated, uncomplicated cases, current data do not support them as a standard recommendation. Prompt diagnosis and tailored surgical intervention offer the best outcomes for pediatric TAWH cases.
Ethical approval
The parents of the patients gave their written informed consent for this report to be published.
Source of funding
The authors declare the study received no funding.
Conflict of interest
The authors declare that there is no conflict of interest.
References
- Theodorou CM, Stokes SC, Beres AL. Traumatic abdominal wall hernia in children: a systematic review. J Surg Res 2021; 262: 181-189. https://doi.org/10.1016/j.jss.2020.12.068
- Navarro-Nuño DE, de Jesús Valdez-Pereira H, Cervantes-Nuño AV, Dorado-Hernández E, Torres-Salazar QL. Traumatic abdominal wall hernia: case report of atypical origin. Int J Surg Case Rep 2023; 110: 108780. https://doi.org/10.1016/j.ijscr.2023.108780
- Selby CD. Direct abdominal hernia of traumatic origin. Jama 1906; 18: 1485-1486. https://doi.org/10.1001/jama.1906.25210180061002c
- Landry RM. Traumatic hernia. Am J Surg 1956; 91: 301-302. https://doi.org/10.1016/0002-9610(56)90427-5
- Yadav S, Jain SK, Arora JK, et al. Traumatic abdominal wall hernia: delayed repair: advantageous or taxing. Int J Surg Case Rep 2013; 4: 36-39. https://doi.org/10.1016/j.ijscr.2012.10.004
- Dennis RW, Marshall A, Deshmukh H, et al. Abdominal wall injuries occurring after blunt trauma: incidence and grading system. Am J Surg 2009; 197: 413-417. https://doi.org/10.1016/j.amjsurg.2008.11.015
- Belgers HJ, Hulsewé KWE, Heeren PAM, Hoofwijk AGM. Traumatic abdominal wall hernia: delayed presentation in two cases and a review of the literature. Hernia 2005; 9: 388-391. https://doi.org/10.1007/s10029-005-0338-6
- Martinez BD, Stubbe N, Rakower SR. Delayed appearance of traumatic ventral hernia: a case report. J Trauma 1976; 16: 242-243. https://doi.org/10.1097/00005373-197603000-00012
- Schmidt MS, Rosenberg J, Tolver MA. Traumatic bicycle handlebar hernia in children: a systematic review. Dan Med J 2018; 65: A5433.
- Cheung R, Shukla M, Akers KG, Farooqi A, Sethuraman U. Bicycle handlebar injuries - a systematic review of pediatric chest and abdominal injuries. Am J Emerg Med 2022; 51: 13-21. https://doi.org/10.1016/j.ajem.2021.09.043
- Steenburg SD, Padilla-Jones B, Lee JT, et al. Traumatic abdominal wall injuries-a primer for radiologists. Emerg Radiol 2021; 28: 361-371. https://doi.org/10.1007/s10140-020-01842-w
- Netto FACS, Hamilton P, Rizoli SB, et al. Traumatic abdominal wall hernia: epidemiology and clinical implications. J Trauma 2006; 61: 1058-1061. https://doi.org/10.1097/01.ta.0000240450.12424.59
- Burt BM, Afifi HY, Wantz GE, Barie PS. Traumatic lumbar hernia: report of cases and comprehensive review of the literature. J Trauma 2004; 57: 1361-1370. https://doi.org/10.1097/01.ta.0000145084.25342.9d
- Vu TND, Klinkner DB. Traumatic abdominal wall hernia with evisceration secondary to handlebar injury. J Pediatr Surg Case Rep 2019; 47. https://doi.org/10.1016/j.epsc.2019.
- Hernandez Cervantes BY, Martínez Lopez D, Guzman Lambert R, Rodríguez Gonzalez M, Meah M. Acute traumatic abdominal wall hernia-value of the physical examination: case report. J Surg Case Rep 2021; 2021: rjab314. https://doi.org/10.1093/jscr/rjab314
- Akbaba S, Gündoğdu RH, Temel H, Oduncu M. Traumatic abdominal wall hernia: early or delayed repair? Indian J Surg 2015; 77: 963-966. https://doi.org/10.1007/s12262-014-1083-9
- Arenaza Choperena G, Cuetos Fernández J, Gómez Usabiaga V, Ugarte Nuño A, Rodriguez Calvete P, Collado Jiménez J. Abdominal trauma. Radiologia 2023; 65: 32-41. https://doi.org/10.1016/j.rxeng.2022.09.011
- Talutis SD, Muensterer OJ, Pandya S, McBride W, Stringel G. Laparoscopic-assisted management of traumatic abdominal wall hernias in children: case series and a review of the literature. J Pediatr Surg 2015; 50: 456-461. https://doi.org/10.1016/j.jpedsurg.2014.10.020
- Damschen DD, Landercasper J, Cogbill TH, Stolee RT. Acute traumatic abdominal hernia: case reports. J Trauma 1994; 36: 273-276. https://doi.org/10.1097/00005373-199402000-00026
- Riesberg JC, Gurney JM, Morgan M, et al. The management of abdominal evisceration in tactical combat casualty care: TCCC Guideline Change 20-02. J Spec Oper Med 2021; 21: 138-142. https://doi.org/10.55460/9U6S-1K7M
- Suhardja TS, Atalla MA, Rozen WM. Complete abdominal wall disruption with herniation following blunt injury: case report and review of the literature. Int Surg 2015; 100: 531-539. https://doi.org/10.9738/INTSURG-D-14-00079.1
- Goliath J, Mittal V, McDonough J. Traumatic handlebar hernia: a rare abdominal wall hernia. J Pediatr Surg 2004; 39: 20-22. https://doi.org/10.1016/j.jpedsurg.2004.06.039
- Mitchell PJ, Green M, Ramesh AN. Handlebar hernia in children. Emerg Med J 2011; 28: 439-440. https://doi.org/10.1136/emj.2009.089870
- Drago SP, Nuzzo M, Grassi GB. Traumatic ventral hernia: report of a case, with special reference to surgical treatment. Surg Today 1999; 29: 1111-1114. https://doi.org/10.1007/s005950050655
- Rowell EE, Chin AC. Laparoscopic repair of traumatic abdominal wall hernia from handlebar injury. J Pediatr Surg 2011; 46: 9-12. https://doi.org/10.1016/j.jpedsurg.2011.01.031
- Litton K, Izzidien AY, Hussien O, Vali A. Conservative management of a traumatic abdominal wall hernia after a bicycle handlebar injury (case report and literature review). J Pediatr Surg 2008; 43: 31-32. https://doi.org/10.1016/j.jpedsurg.2007.12.059
Copyright and license
Copyright © 2026 The Author(s). This is an open access article distributed under the Creative Commons Attribution License (CC BY), which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is properly cited.