
Abstract
Background. This study retrospectively evaluates the microbiological profile, antibiotic susceptibility patterns, and the effectiveness of empirically initiated antibiotic therapies in children with perforated appendicitis, based on intraoperative peritoneal fluid culture and antibiogram results.
Methods. A total of 154 pediatric patients (97 boys, 57 girls; mean age 9.15 ± 4.08 years) underwent surgery for perforated appendicitis between 2014 and 2020. Before surgery, patients received one of three empirical antibiotic combinations: (1) Ampicillin/sulbactam, metronidazole, and amikacin; (2) ceftriaxone and metronidazole; (3) cefotaxime and metronidazole. Peritoneal fluid samples collected intraoperatively were cultured, and microbial growth and susceptibility profiles were analyzed.
Results. A total of 167 strains were isolated. The most common microorganisms were Escherichia coli (79.0%), Pseudomonas aeruginosa (13.8%), Klebsiella pneumoniae (2.4%), Enterobacter cloacae (1.8%), Enterococcus raffinosus (2.4%), and Staphylococcus hominis (0.6%). Before surgery, Combination 1 was administered to 97 patients (63.0%), Combination 2 to 38 patients (24.7%), and Combination 3 to 19 patients (12.3%). Antibiotic susceptibility of the isolated microorganisms was as follows. E. coli: ampicillin/sulbactam 23%, ceftriaxone 60%, cefotaxime 92%, amikacin 99%. P. aeruginosa: ampicillin/sulbactam 8%, ceftriaxone 16%, cefotaxime 0%, amikacin 99%. K. pneumoniae: ceftriaxone 75%, cefotaxime 75%, amikacin 100%. E. raffinosus: ceftriaxone 33%, cefotaxime 100%, amikacin 100%. Postoperative modification of empirical therapy was required in 102 cases (66.2%)
Conclusions. High resistance rates to commonly used empirical antibiotics were observed among isolated microorganisms, highlighting the need for regular revision of empirical treatment protocols and greater reliance on intraoperative culture results in pediatric perforated appendicitis.
Keywords: empirical antibiotic therapy, peritoneal fluid microbiology, antibiotic resistance patterns, postoperative infectious complications, antimicrobial stewardship programs
Introduction
Perforated appendicitis is the most common cause of community-acquired intra-abdominal infections in children.1,2 The optimal management of perforated appendicitis in children remains controversial.3 Urgent appendectomy has traditionally been considered the standard approach.4-6 However, emergency surgery may be technically challenging due to an edematous and fragile appendix and the surrounding intestinal loops and tissues. A second reasonable option is initial nonoperative management with broad-spectrum antibiotics to stabilize the patient and avoid a troublesome operation.7
Timely initiation of empirical antibiotic therapy is critical, as delays increase the risk of postoperative complications such as intra-abdominal abscesses. Antibiotic selection varies across institutions and surgeons, requiring a balance between antimicrobial resistance, clinical efficacy, and cost.5,8-12 Although the spectrum of pathogens in perforated appendicitis has remained relatively consistent, susceptibility patterns differ by region and evolve over time, underscoring the importance of local microbiological surveillance.1,2,11-15
In our clinic, empirical antibiotic regimens have long been guided by the recommendations of the Surgical Infection Society and the Infectious Diseases Society of America.3These guidelines recommend broad-spectrum coverage targeting aerobic and anaerobic Gram-negative organisms, which are the predominant pathogens in perforated appendicitis. Accordingly, our empirical regimens include ampicillin/sulbactam, amikacin, and metronidazole; ceftriaxone and metronidazole; or cefotaxime and metronidazole. The choice among these combinations is influenced by local resistance patterns, surgeon experience, drug availability, and cost considerations.
In clinical practice, the attending pediatric surgeon selects the empirical regimen based on disease severity, hemodynamic status, and perceived risk of resistant organisms. However, an increase in postoperative complications in recent years has led to more frequent culture-guided antibiotic modifications.8,10,13
This study retrospectively evaluates intra-abdominal fluid culture and antibiogram results obtained during surgery in children with perforated appendicitis, with the aim of characterizing the microbiological profile, determining antibiotic susceptibility patterns, and assessing their impact on empirical antibiotic therapy. Our central hypothesis is that intraoperative peritoneal fluid cultures improve empirical antibiotic selection by identifying resistance to commonly used agents, thereby reducing postoperative complications.
Materials and Methods
Study design and participants
This retrospective study included 154 pediatric patients who underwent surgery for perforated appendicitis between January 2014 and December 2020 at the Pediatric Surgery Clinic of Adıyaman Training and Research Hospital. Intra-abdominal fluid samples were collected during surgery for microbiological analysis.
Exclusion criteria were the absence of intra-abdominal fluid culture, negative culture results, non-operative management, uncomplicated acute appendicitis, hospitalization within the previous three months, and preoperative antibiotic use.
This study was approved by the Ethics Committee for Non-Invasive Clinical Research at Adıyaman University Faculty of Medicine (decision number 2020/7-20, dated 21.07.2020). Written informed consent was obtained from the parents of all participants.
Diagnostic criteria
The diagnosis of perforated appendicitis was based on clinical history, physical examination, laboratory findings (white blood cell count [WBC, ×10³/μL] and C-reactive protein [CRP, mg/dL]), imaging studies, and intraoperative confirmation.2,5 Imaging modalities included ultrasonography (USG) and/or intravenous (IV) contrast-enhanced computed tomography (CT). Imaging findings suggestive of perforation included peri-appendiceal fluid, irregular or disrupted appendix wall, contaminated pericecal appearance, and free intraperitoneal air. Intraoperative confirmation included visualization of a perforated appendix wall, intra-abdominal fecaliths, or abscesses formation.16
Data collection
Patients’ medical records were retrospectively reviewed using the KarMed Health Information Management System (Version 1.2.48.299). Data included patient age, sex, pre-antibiotic WBC and CRP levels, imaging modality, empirical antibiotic regimen, time from diagnosis to surgery, surgical technique, intra-abdominal fluid culture and antibiogram results, postoperative antibiotic modifications and indications, length of hospital stay, and postoperative complications (intra-abdominal abscess, surgical site infection [SSI]) within 30 days after surgery.
Procedures and antibiotic regimens
All patients received IV fluids and antibiotics after diagnosis. Preoperative antibiotics were administered within 1 hour of diagnosis according to institutional protocol. Empirical antibiotic therapy was selected by the attending pediatric surgeon based on clinical severity, risk of resistant organisms, local susceptibility patterns, drug availability and cost considerations. Broader regimens (Combination 1) were typically preferred for patients with more severe presentations. Empirical antibiotic therapy consisted of one of the following combinations:
Combination 1: Ampicillin/sulbactam (Sulbaksit, Tüm Ekip İlaç, 2002), metronidazole (Metrosel, OSEL İlaç, 2003), and amikacin (Amikaver, OSEL, 1999).
Combination 2: Ceftriaxone (Desefin, Deva Holding A.Ş, 2006) and metronidazole.
Combination 3: Cefotaxime (Eqitax, Tüm Ekip İlaç, 2003) and metronidazole.
Dosages were as follows: ampicillin/sulbactam 150 mg/kg/day in four doses IV, metronidazole 30 mg/kg/day in three doses IV, amikacin 15 mg/kg/day in two doses IV, ceftriaxone 100 mg/kg/day in two doses IV, and cefotaxime 100 mg/kg/day in three doses IV.
To ensure clarity and reproducibility, patients were categorized into three groups based on the empirical antibiotic regimen administered prior to surgery. Group 1 consisted of patients who received Combination 1; Group 2 included those treated with Combination 2; and Group 3 included patients who received Combination 3.
All patients underwent open appendectomy within 8 hours of diagnosis, and no laparoscopic procedures were performed. During surgery, 1-10 mL of peri-appendiceal fluid was aspirated using a sterile syringe. The abdominal cavity was irrigated with warm sterile saline until clear. A soft or Penrose drain was placed in all cases and removed on postoperative days 3–5. Samples drawn into syringes were inoculated into aerobic and anaerobic blood culture media (Pediatric blood culture vials, BD, USA) and transported to the microbiology culture laboratory. Bacterial identification and antibiotic susceptibility testing were performed using an automated system (Phoenix 100, BD, USA). Results, including minimum inhibitory concentration (MIC) values and extended-spectrum beta-lactamase (ESBL) positivity, were reported within 1-5 days.
Post-operative empirical antibiotic therapy was modified based on poor clinical progress, laboratory findings (unresolved WBC and CRP levels), culture and antibiogram results, or complications such as intra-abdominal abscesses and SSIs. Unresolved WBC and CRP levels were defined as: WBC remaining above 12 ×10³/μL or increasing compared with the previous day, and/or CRP remaining failing to show a downward trend within 48–72 hours postoperatively.
Definitions
Poor clinical progress was defined as persistent fever (>38°C), abdominal pain, vomiting, diarrhea, inability to tolerate oral intake, abdominal distention, rising WBC/CRP levels, pre-operative intra-abdominal abscess, diffuse peritonitis, or severe intestinal adhesions.3
Post-operative patients with deteriorating general conditions, fever, abdominal pain, vomiting, diarrhea, or elevated WBC and CRP levels were evaluated for intra-abdominal abscess via USG by a radiologist. Intra-abdominal abscesses were treated with antibiotics, and when necessary, USG-guided percutaneous drainage.
Surgical site infections were defined according to the Centers for Disease Control and Prevention (CDC) criteria, including superficial, deep, or organ/space infections occurring within 30 days postoperatively.17
Statistical analysis
Statistical analyses were performed using SPSS version 22.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics were used to summarize demographic characteristics, laboratory values, microbiological findings, and postoperative outcomes. Continuous variables were expressed as mean ± standard deviation (SD) or median (range), depending on distribution. Categorical variables were expressed as frequencies and percentages.
Normality of distribution for continuous variables was assessed using the Shapiro–Wilk test. For comparisons Student’s t-test was applied to normally distributed data, while the Mann–Whitney U test was used for non-normally distributed data. Categorical variables were compared using the chi-square test or Fisher’s exact test, as appropriate. A p-value of <0.05 was considered statistically significant.
No formal power analysis was performed prior to the study; however, the sample size was considered adequate for descriptive and comparative analyses. Although Groups 2 and 3 had relatively small sample sizes, comparative analyses were performed across the three empirical antibiotic regimens for postoperative outcomes, including intra-abdominal abscess and surgical site infection rates. Antibiotic resistance patterns were evaluated descriptively based on culture results, without formal statistical comparison between empirical treatment groups.
A post-hoc power analysis was performed to evaluate the ability of the study to detect differences in postoperative intra-abdominal abscess and SSI rates among the three empirical antibiotic regimen groups. Given the observed effect sizes and the sample distribution (Group 1: n=97, Group 2: n=38, Group 3: n=19), the statistical power for detecting small-to-moderate differences between groups was limited (<0.60), particularly for Groups 2 and 3 due to their smaller sample sizes. Therefore, non-significant findings in these comparisons should be interpreted with caution.
Results
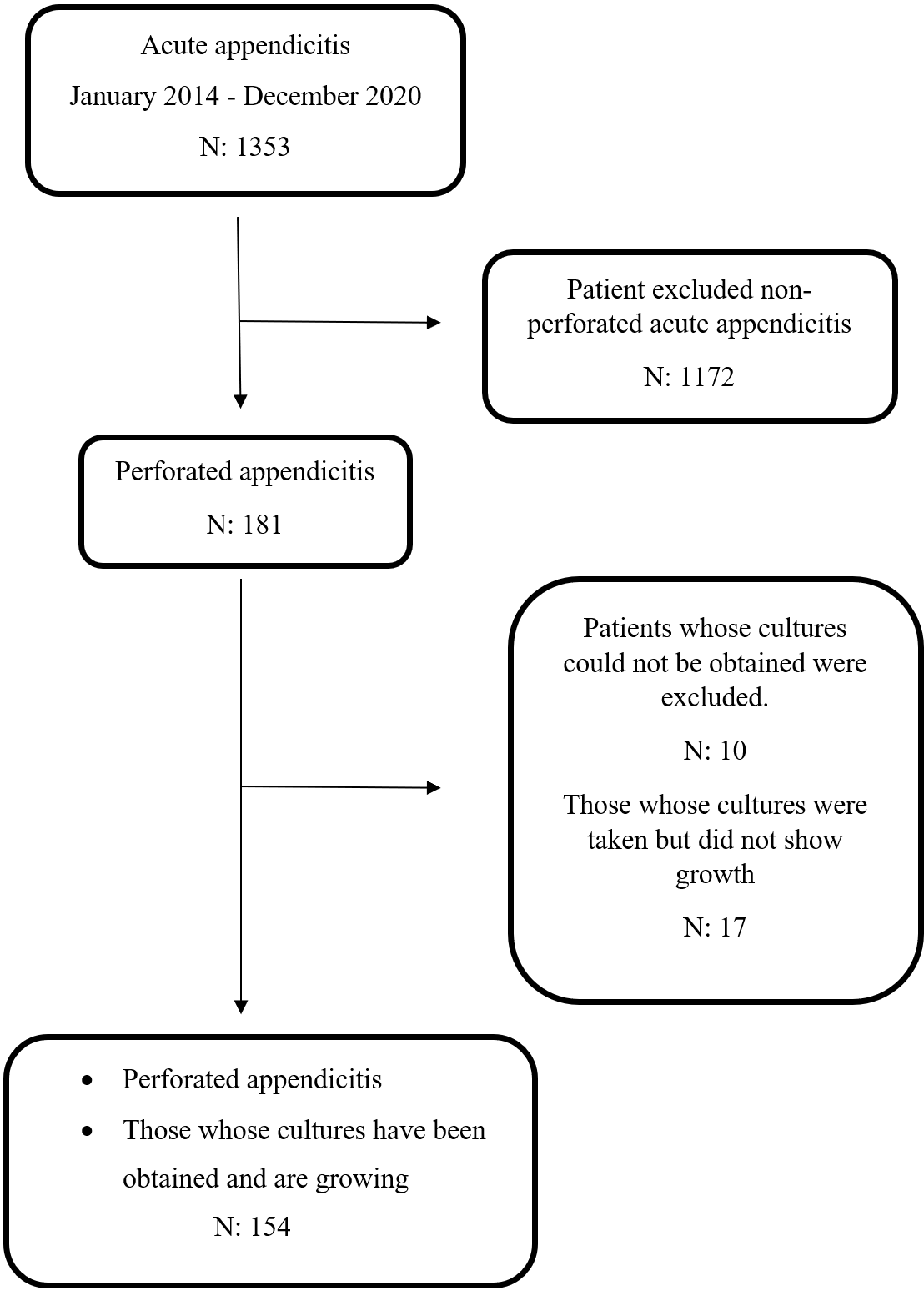
Between January 2014 and December 2020, 1353 cases of acute appendicitis were treated at Adıyaman Training and Research Hospital. Of these, 181 (13.4%) had perforated appendicitis. Intra-abdominal fluid cultures were obtained in 171 (94.5%) cases, and bacterial growth was detected in 154 (90.1%) cases, all of whom were included in this study (Fig. 1).
Patient characteristics
Among the 154 cases, 97 (63%) were boys and 57 (37%) were girls, with a mean age of 9.15 ± 4.08 years. The mean length of hospital stay was 9.94 ± 3.93 days. Demographic characteristics and preoperative laboratory values are summarized in Table I.
| CRP: C-reactive protein, F: female, M: male, SD: standard deviation, WBC: white blood cell. | |
| Table I. Demographic, and microbiological characteristics of the patients (N=154). | |
| Age (years), mean ± SD |
|
| Sex (F/M), n (%) |
|
| Preoperative WBC count (103/µL), mean ± SD |
|
| Preoperative CRP (mg/dL), median (range) |
|
| Length of hospital stay (day), mean ± SD |
|
| İntraabdominal abscess, n (%) |
|
| Surgical site infection, n (%) |
|
| Distribution of microorganisms isolated in peritoneal fluid culture, n (%) | |
| E. coli |
|
| P. aeruginosa |
|
| K. pneumoniae |
|
| E. raffinosus |
|
| E. cloacae |
|
| S. hominis |
|
Microbiological findings
A total of 167 bacterial strains were isolated from the intra-abdominal fluid cultures. Polymicrobial growth was observed in 13 patients (8.4%). The most frequently isolated microorganisms were: Escherichia coli (132, 79.0%), Pseudomonas aeruginosa (23, 13.8%), Klebsiella pneumoniae (4, 2.4%), Enterobacter cloacae (3, 1.8%), Enterococcus raffinosus (4, 2.4%), Staphylococcus hominis (1, 0.6%) (Table I.). ESBL production was detected in 12 E. coli isolates (9.1%) and 1 K. pneumoniae isolate (25%).
Antibiotic susceptibility
Three empirical antibiotic combinations were used. 97 patients (63.0%): ampicillin/sulbactam, metronidazole, and amikacin, 38 patients (24.7%): ceftriaxone and metronidazole, 19 patients (12.3%): cefotaxime and metronidazole.
The susceptibility patterns of the most common isolates are shown in Table II. E. coli isolates demonstrated low susceptibility to ampicillin/sulbactam (23%) and ceftriaxone (60%) compared to cefotaxime (92%) and amikacin (99%). (p < 0.001). P. aeruginosa isolates demonstrated low susceptibility to ampicillin/sulbactam (8%), ceftriaxone (16%), and cefotaxime (0%) but high susceptibility to amikacin (99%), meropenem (92%), and piperacillin/tazobactam (73%). (p < 0.001). Susceptibility to meropenem was significantly higher than to piperacillin/tazobactam (p < 0.05). K. pneumoniae isolates demonstrated no susceptibility to ampicillin/sulbactam (0%). moderate susceptibility to ceftriaxone (75%) and cefotaxime (75%), and high susceptibility to amikacin (100%) and meropenem (100%) (p < 0.001). Piperacillin/tazobactam showed lower susceptibility (75%) compared to ceftriaxone and cefotaxime.
| AMK: amikacin; CAZ: ceftazidime; CN: gentamicin; CRO: ceftriaxone; CTX: cefotaxime; CXA: cefuroxime; ETP: ertapenem; IPM: imipenem; MEM: meropenem; SAM: ampicillin-sulbactam; TZP: piperacillin-tazobactam; VA: vancomycin. | |||||||||||||
| Table II. Antimicrobial susceptibility rates of microorganisms isolated from peritoneal fluid. | |||||||||||||
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| E. coli |
|
|
|
|
|
|
|
|
|
|
|
|
|
| P. aeruginosa |
|
|
|
|
|
|
|
|
|
|
|
|
|
| K. pneumoniae |
|
|
|
|
|
|
|
|
|
|
|
|
|
| E. raffinosus |
|
|
|
|
|
|
|
|
|
|
|
|
|
| E. cleocae |
|
|
|
|
|
|
|
|
|
|
|
|
|
| S. hominis |
|
|
|
|
|
|
|
|
|
|
|
|
|
Post-operative outcomes
Empirical antibiotic therapy was modified in 102 cases (66.2%) due to resistance to at least one antibiotic in the empirical regimen, poor clinical progress, development of intra-abdominal abscesses, or SSIs (Table III).
| Data expressed as number (percentage). SSI: surgical site infection. | ||||||
| Table III. Postoperative modification of empirical antibiotic therapy and reasons for change. | ||||||
| Empirical regimen group |
patients |
|
|
|
|
|
| Group 1 |
|
|
|
|
|
|
| Group 2 |
|
|
|
|
|
|
| Group 3 |
|
|
|
|
|
|
| Total |
|
|
|
|
|
|
Intra-abdominal abscess developed post-operatively in 31 cases (20.1%). The median time to abscess formation was 10 days (range 5–18). Twenty patients (64,5%) already had intra-abdominal abscess at the time of surgery. The intra-abdominal fluid cultures results among abscess cases yielded E. coli in 24 cases (77.4%), P. aeruginosa in 5 cases (16.1%), K. pneumoniae in 1 case (3.2%), and E. cloacae in 1 case (3.2%).
Postoperative abscess formation showed no meaningful variation among the empirical antibiotic regimens, occurring in 20/97 (20.6%) of patients in Group 1, 7/38 (18.4%) in Group 2, and 4/19 (21.0%) in Group 3, with no statistically significant differences observed (p > 0.05). Among patients with abscesses where E. coli was isolated, empirical therapy included ampicillin/sulbactam, amikacin, and metronidazole in 15 cases; ceftriaxone and metronidazole in 5 cases; and cefotaxime and metronidazole in 4 cases. Resistance to empirical therapy was observed as follows: ampicillin/sulbactam (11 strains resistant, 4 susceptible), ceftriaxone (3 strains susceptible, 2 resistant), and cefotaxime (2 strains susceptible, 2 resistant). Among patients with abscesses caused by P. aeruginosa, all 5 cases showed resistance to empirical therapy (ampicillin/sulbactam in 3 cases, ceftriaxone in 2 cases). Resistance to ceftriaxone was noted in one case with K. pneumoniae. Resistance to cefotaxime was observed in one case with E. cloacae. Overall, 22 (71.0%) of the patients with abscesses had isolates resistant to at least one antibiotic in the empirical regimen. The frequency of resistant strains was significantly higher in patients who developed intra-abdominal abscesses (p < 0.01).
Antibiotic therapy was changed post-abscess development in 27 cases (87.1%). Changes included meropenem (16 cases), imipenem (3 cases), ceftriaxone (2 cases), piperacillin/tazobactam (2 cases), trimethoprim-sulfamethoxazole (2 cases), cefoperazone/sulbactam (1 case), and vancomycin + meropenem (1 case). Abscess resolution was achieved with antibiotics alone in 30 cases (96.8%), and with percutaneous drainage plus antibiotics in 1 case (3.2%).
Surgical site infections developed in 39 patients (25%). SSI rates did not differ significantly between antibiotic regimen groups (p > 0.05). Despite resistance to empirical antibiotic therapy in 31 SSI cases (79.5%), antibiotic modification was required in only 4 cases (10.2%). The most patients improved with daily local wound care and drainage.
Discussion
The Infectious Diseases Society of America’s 2024 Clinical Practice Guideline emphasizes the importance of obtaining intra-abdominal cultures to guide antimicrobial therapy for complicated intra-abdominal infections.18Consistent with these recommendations, intra-abdominal fluid cultures were obtained in 94.5% of cases in our study, highlighting their routine use in clinical practice. Current guidelines advise avoiding empirical antibiotics with resistance rates exceeding 10%–20%,3,11,19 underscoring the importance of local susceptibility data in optimizing treatment strategies.
Our study identified E. coli as the most frequent isolate (79%), followed by P. aeruginosa (13.8%), K. pneumoniae (2.4%), and E. raffinosus (2.4%), consistent with previous studies from Türkiye and Europe.1,8,9 In Türkiye, studies from İzmir, Elazığ, Istanbul, and Adıyaman similarly report E. coli as the predominant pathogen, with P. aeruginosa ranking as the second or the third most common isolate.,8,9,20 Regional variability in ESBL positivity further highlights the need for center-specific microbiological surveillance.
Regarding antibiotic susceptibility, our study found E. coli to be highly resistant to ampicillin/sulbactam (23%) and moderately susceptible to ceftriaxone (60%). Antibiotics with over 90% susceptibility included cefotaxime, carbapenems, amikacin, and gentamicin. These results align with national and European data, which similarly report low activity of ampicillin/sulbactam and high effectiveness of carbapenems and aminoglycosides.1,8,9
The susceptibility of P. aeruginosa to the empirically used antibiotics was below 16%, except for amikacin (99%). Antibiotics with over 90% effectiveness against this agent were carbapenems amikacin, and gentamicin. Similar results were reported by Turel and Tartar, who found no susceptibility to ampicillin/sulbactam and >90% activity for imipenem and amikacin.8,9 Lob et al. also reported high susceptibility to imipenem, cefepime, ceftazidime, and amikacin.1 Notably, piperacillin/tazobactam was less effective in our cohort (<75%) compared to other reports, emphasizing regional differences.1,8
K. pneumoniae isolates in our study showed ≤75% susceptibility to most empirically used antibiotics, except for amikacin (100%) and carbapenems (>90%). These results are consistent with previous studies reporting low susceptibility to ceftriaxone and cefotaxime but high susceptibility to carbapenems.1,8 Notably, piperacillin/tazobactam susceptibility was lower in our study (<80%) compared with >90% in other reports, again emphasizing the need for continuous local surveillance.
Although amikacin showed 98% susceptibility to all isolated microorganisms, its use as monotherapy is limited by the polymicrobial nature of perforated appendicitis and resistance to companion agents such as ampicillin/sulbactam.1 The guidelines by the Surgical Infection Society and the Infectious Diseases Society of America recommend gentamicin and tobramycin as part of combination therapy.3
Based on these findings, our center has initiated a review of empirical antibiotic protocols, with consideration of replacing ampicillin/sulbactam, metronidazole, amikacin, and ceftriaxone, metronidazole combinations with cefotaxime, metronidazole combination
Postoperative intra-abdominal abscesses occurred in 20.1% of cases, consistent with studies previously reported rates of 14%–20%.14,21,22 Importantly, 71.0% of abscess cases involved pathogens resistant to at least one antibiotic in the empirical regimen, highlighting the clinical relevance of culture-guided therapy. Abscess rates did not differ significantly between the three empirical antibiotic groups, suggesting that resistance patterns rather than the specific empirical regimen may play a more decisive role in abscess formation.
Surgical site infections developed in 25.3% of patients, predominantly caused by E. coli (79.5%). Most cases were successfully managed with local wound care, and only a minority required antibiotic modification, consistent with previous studies.8
This retrospective single-center study has several limitations. The relatively small sample size in Groups 2 and 3 limited the statistical power of between-group comparisons. Additionally, patients with more severe clinical presentations were more likely to receive broader empirical regimens (e.g., Combination 1). This may have introduced confounding by indication. As a result, treatment failures associated with certain regimens may be overestimated. Other limitations include the absence of multivariate analysis to adjust for confounders, the lack of a matched control group (e.g., non-perforated appendicitis), and the potential influence of clinical variables such as symptom duration, timing of admission, comorbidities, drain use, and operative technique. Future multicenter prospective studies are needed to validate these findings and refine empirical antibiotic strategies.
Conclusions
The microorganisms isolated from intra-abdominal cultures in pediatric perforated appendicitis demonstrated high resistance to commonly recommended empirical agents such as ampicillin/sulbactam, ceftriaxone, and piperacillin/tazobactam. These findings underscore the necessity of regularly updating empirical antibiotic protocols based on intraoperative culture results and local resistance patterns. Tailoring postoperative antibiotic modifications according to both clinical response and antibiogram results may improve treatment effectiveness and reduce postoperative complications.
Ethical approval
The study was approved by the Ethics Committee for Non-Invasive Clinical Research at Adıyaman University Faculty of Medicine (dated 21.07.2020, decision number 2020/7-20).
Source of funding
The authors declare the study received no funding.
Conflict of interest
The authors declare that there is no conflict of interest.
References
- Lob SH, Badal RE, Hackel MA, Sahm DF. Epidemiology and antimicrobial susceptibility of gram-negative pathogens causing intra-abdominal infections in pediatric patients in Europe-SMART 2011-2014. J Pediatric Infect Dis Soc 2017; 6: 72-79. https://doi.org/10.1093/jpids/piv109
- Aiyoshi T, Masumoto K, Tanaka N, et al. Optimal first-line antibiotic treatment for pediatric complicated appendicitis based on peritoneal fluid culture. Pediatr Gastroenterol Hepatol Nutr 2021; 24: 510-517. https://doi.org/10.5223/pghn.2021.24.6.510
- Solomkin JS, Mazuski JE, Bradley JS, et al. Diagnosis and management of complicated intra-abdominal infection in adults and children: guidelines by the Surgical Infection Society and the Infectious Diseases Society of America. Clin Infect Dis 2010; 50: 133-164. https://doi.org/10.1086/649554
- Dabaja-Younis H, Farah H, Miron R, et al. The intraperitoneal bacteriology and antimicrobial resistance in acute appendicitis among children: a retrospective cohort study between the years 2007-2017. Eur J Pediatr 2021; 180: 2091-2098. https://doi.org/10.1007/s00431-021-03994-4
- Kitahara H, Park Y, Seharada K, Yoshimura M, Horiuchi A, Karasawa Y. Culture-based bacterial evaluation of the appendix lumen and antibiotic susceptibility of acute appendicitis in Japan: a single-center retrospective analysis. Medicine (Baltimore) 2024; 103: e39037. https://doi.org/10.1097/MD.0000000000039037
- Tan A, Rouse M, Kew N, Qin S, La Paglia D, Pham T. The appropriateness of ceftriaxone and metronidazole as empirical therapy in managing complicated intra-abdominal infection-experience from Western Health, Australia. PeerJ 2018; 6: e5383. https://doi.org/10.7717/peerj.5383
- Vaos G, Dimopoulou A, Gkioka E, Zavras N. Immediate surgery or conservative treatment for complicated acute appendicitis in children? A meta-analysis. J Pediatr Surg 2019; 54: 1365-1371. https://doi.org/10.1016/j.jpedsurg.2018.07.017
- Turel O, Mirapoglu SL, Yuksel M, Ceylan A, Gultepe BS. Perforated appendicitis in children: antimicrobial susceptibility and antimicrobial stewardship. J Glob Antimicrob Resist 2019; 16: 159-161. https://doi.org/10.1016/j.jgar.2018.09.015
- Tartar T, Sağmak-Tartar A, Saraç M, Bakal Ü, Akbulut A, Kazez A. Does microbial resistance profile change in community-based intra-abdominal infections? Evaluation of the culture results of patients with appendicitis. Turk J Pediatr 2018; 60: 520-526. https://doi.org/10.24953/turkjped.2018.05.008
- Obinwa O, Casidy M, Flynn J. The microbiology of bacterial peritonitis due to appendicitis in children. Ir J Med Sci 2014; 183: 585-591. https://doi.org/10.1007/s11845-013-1055-2
- Brits E, Kruger E, Fivaz K, et al. Type and antibiotic susceptibility of bacteria cultured in paediatric acute appendicitis. S Afr J Infect Dis 2025; 40: 689. https://doi.org/10.4102/sajid.v40i1.689
- Gerber F, Joseph JM, Crisinel PA, Andrey V. Evidence-based optimisation of empirical antibiotic regimens in paediatric complicated appendicitis: a retrospective study of 94 patients. Swiss Med Wkly 2022; 152: w30222. https://doi.org/10.4414/smw.2022.w30222
- Cantón R, Loza E, Aznar J, et al. Monitoring the antimicrobial susceptibility of Gram-negative organisms involved in intraabdominal and urinary tract infections recovered during the SMART study (Spain, 2016 and 2017). Rev Esp Quimioter 2019; 32: 145-155.
- Garzon-González LN, Padilla LT, Patiño F, et al. Association between bacterial resistance profile and the development of intra-abdominal abscesses in pediatric patients with perforated appendicitis: cohort study. Pediatr Surg Int 2023; 40: 18. https://doi.org/10.1007/s00383-023-05570-3
- Kakar M, Reinis A, Kroica J, et al. Microbiota assessment of pediatric simple and complex acute appendicitis. Medicina (Kaunas) 2022; 58: 1144. https://doi.org/10.3390/medicina58091144
- Holcomb GW, St Peter SD. Current management of complicated appendicitis in children. Eur J Pediatr Surg 2012; 22: 207-212. https://doi.org/10.1055/s-0032-1320016
- Berríos-Torres SI, Umscheid CA, Bratzler DW, et al. Centers for disease control and prevention guideline for the prevention of surgical site infection, 2017. JAMA Surg 2017; 152: 784-791. https://doi.org/10.1001/jamasurg.2017.0904
- Bonomo RA, Chow AW, Edwards MS, et al. 2024 Clinical Practice Guideline update by the Infectious Diseases Society of America on complicated intra-abdominal infections: risk assessment, diagnostic imaging, and microbiological evaluation in adults, children, and pregnant people. Clin Infect Dis 2024; 79: 81-87. https://doi.org/10.1093/cid/ciae346
- Jeon HG, Ju HU, Kim GY, Jeong J, Kim MH, Jun JB. Bacteriology and changes in antibiotic susceptibility in adults with community-acquired perforated appendicitis. PLoS One 2014; 9: e111144. https://doi.org/10.1371/journal.pone.0111144
- Celik A, Ergün O, Ozcan C, Aldemir H, Balik E. Is it justified to obtain routine peritoneal fluid cultures during appendectomy in children? Pediatr Surg Int 2003; 19: 632-634. https://doi.org/10.1007/s00383-003-0978-5
- Fraser JD, Aguayo P, Leys CM, et al. A complete course of intravenous antibiotics vs a combination of intravenous and oral antibiotics for perforated appendicitis in children: a prospective, randomized trial. J Pediatr Surg 2010; 45: 1198-1202. https://doi.org/10.1016/j.jpedsurg.2010.02.090
- Hamdy RF, Handy LK, Spyridakis E, et al. Comparative effectiveness of ceftriaxone plus metronidazole versus anti-pseudomonal antibiotics for perforated appendicitis in children. Surg Infect (Larchmt) 2019; 20: 399-405. https://doi.org/10.1089/sur.2018.234
Copyright and license
Copyright © 2026 The Author(s). This is an open access article distributed under the Creative Commons Attribution License (CC BY), which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is properly cited.









