
Graphical Abstract
Abstract
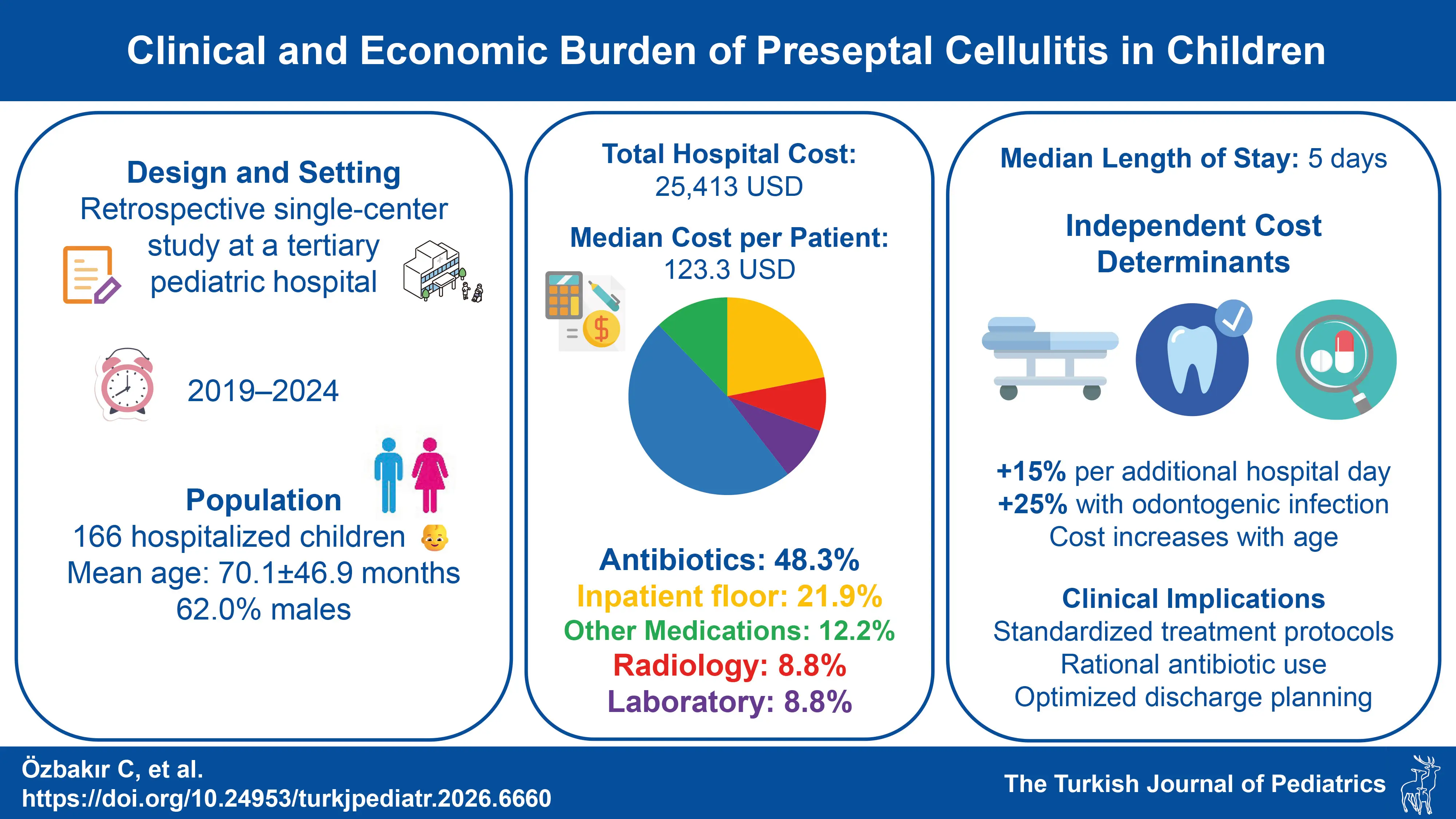
Background. Children diagnosed with preseptal cellulitis frequently require hospitalization, leading to both clinical management challenges and substantial healthcare-related costs. The condition often necessitates intravenous antibiotic therapy, radiological imaging, laboratory tests, consultations, and inpatient care, which collectively contribute to the overall economic burden. However, data on the clinical characteristics and cost distribution among pediatric patients remain limited. This study aimed to evaluate both the clinical and economic burden of preseptal cellulitis in hospitalized children and to identify the clinical factors influencing healthcare costs.
Methods. This retrospective study included children aged 1 month to 18 years who were hospitalized with a diagnosis of preseptal cellulitis between January 2019 and December 2024. Patients were grouped according to age and presence of predisposing factors. Length of stay, total hospital costs, and cost components were analyzed based on clinical characteristics.
Results. A total of 166 patients were included (mean age: 70.1 ± 46.9 months; 62% male). The most common findings were periorbital swelling (96.4%) and erythema (75.3%). Median length of stay was 5 days, with no significant differences by age, sex, or predisposing factors (p>0.05). However, a strong positive correlation was found between length of stay and total cost (rho=0.775, p<0.001). The total hospital expenditure was 25,412.95 USD, with antibiotics accounting for the largest share (48.3%). Sinusitis and odontogenic infections were significantly associated with higher costs (p=0.007 and p=0.030). In multivariable analysis, length of stay, age, and odontogenic infection emerged as independent determinants of total cost, with costs increasing by approximately 15% per additional hospital day, 0.2% per month of age, and 25% in the presence of odontogenic infection.
Conclusion. Developing standardized treatment protocols and promoting rational antibiotic use are critical for optimizing healthcare resource utilization and preventing antibiotic resistance.
Keywords: antibiotic, hospital cost, sinusitis
Introduction
Preseptal cellulitis is an infection confined to the eyelid and superficial periorbital tissues, without involvement of the globe or orbital contents.1 In contrast, orbital cellulitis involves the tissues posterior to the orbital septum and is associated with more severe outcomes, including vision loss and life-threatening complications.2 While preseptal cellulitis is more frequent and generally milder in children, distinguishing it from orbital cellulitis can be clinically challenging in certain cases.3 When orbital involvement cannot be confidently excluded through physical examination, radiologic imaging, most often contrast-enhanced computed tomography (CT), is required.4 Routine laboratory tests and blood cultures, though commonly used, contribute minimally to diagnosis.5
The cornerstone of treatment is prompt initiation of appropriate antibiotic therapy.6 Factors that may adversely impact clinical outcomes include delayed intervention, immunodeficiency, resistant pathogens, incomplete vaccination, and concurrent sinusitis.7 Management of hospitalized children with preseptal cellulitis, encompassing intravenous antibiotics, imaging, laboratory workup, consultations, and occasional surgical interventions, can result in substantial healthcare expenditures. Previous studies suggest that factors such as sinusitis, age over five years, and development of orbital complications are associated with increased hospital costs.3,8
The absence of standardized guidelines for the diagnosis and management of preseptal cellulitis has led to variability in antibiotic selection and healthcare resource utilization.5 Thus, evaluating factors influencing healthcare costs is essential for optimizing care delivery and promoting cost-effective strategies. This study aims to analyze the clinical and economic burden of pediatric preseptal cellulitis by identifying cost-driving factors and quantifying the contribution of each resource category to overall hospital expenses.
Materials and Methods
This single-center retrospective study was conducted at Dr. Behçet Uz Children’s Hospital, a tertiary care pediatric referral center in İzmir, Türkiye. The study included patients aged between 1 month and 18 years who were hospitalized with a diagnosis of preseptal cellulitis between January 2019 and December 2024. Eligible patients were identified through the hospital’s electronic medical record system. Patients with incomplete medical records or concomitant orbital cellulitis were excluded from the analysis. The medical records of the patients were retrospectively reviewed.
Demographic and clinical data were collected, including age, sex, presenting signs and symptoms (e.g., periorbital swelling, erythema, fever), and predisposing factors (e.g., sinusitis, odontogenic infection, conjunctivitis, insect bite, local trauma). Details regarding the length of stay (LOS), laboratory test results (white blood cell [WBC] count, C-reactive protein [CRP] levels), radiologic imaging (magnetic resonance imaging [MRI] and CT), and administered antibiotic treatments were recorded.
Antibiotic therapy was determined collaboratively by pediatricians and pediatric infectious disease specialists, taking into account the etiologic factors, severity of clinical findings, and duration of response to treatment. There was no standardized institutional protocol for beta-lactam antibiotic selection.
The hospital costs of the patients were extracted from the hospital billing system for cost analysis. The costs were categorized as inpatient floor, radiology, laboratory, antibiotics, and other medications. Other medications included in the cost analysis consisted of non-antibiotic treatments such as isotonic fluids, analgesics, antipyretics, antihistamines, and ophthalmic drops. The hospital costs of the patients were converted to United States Dollars (USD) using the average annual exchange rate of the Turkish Lira to USD for the corresponding year between 2019 and 2024, based on data from the Central Bank of the Republic of Türkiye.
Statistical analyses were performed using SPSS version 25 (IBM Corp., Armonk, NY, USA). Continuous variables were summarized as medians and interquartile ranges (IQR) due to non-parametric distribution, while categorical variables were presented as frequencies and percentages. The Mann–Whitney U test was used to compare non-parametric continuous variables between two independent groups. Spearman’s rank correlation coefficient was used to assess the relationship between the LOS and total hospital cost. A p-value of less than 0.05 was considered statistically significant. In addition, a multivariable generalized linear model with gamma distribution and log link function was used to identify independent factors associated with total hospital cost. The dependent variable was total hospital cost, and the model included age (months), sex, presence of sinusitis, presence of odontogenic infection, and LOS as covariates.
The study was approved by the local ethics committee of Dr. Behçet Uz Children’s Hospital (date: 06.03.2025, decision no: 2025/05-09), in accordance with the Declaration of Helsinki.
Results
Patient characteristics
A total of 166 patients were included (mean age: 70.1 ± 46.9 months; 49.4% ≤5 years; 62.0% male). The most common clinical signs were periorbital swelling (96.4%) and erythema (75.3%). Fever (15.7%), pain (10.2%), and purulent discharge (8.4%) were less frequent. Predisposing factors were identified in 53.6%, with sinusitis (18.1%) and odontogenic infections (12.0%) being most common.
Median WBC count was 10,815/mm³ (IQR: 8,700–13,762), and CRP was 2.4 mg/L (IQR: 0.7–29.8). MRI was performed in 62.7% and CT in 36.7% of cases. All patients received beta-lactam antibiotics, most frequently ceftriaxone (44.6%) and ampicillin-sulbactam (37.4%). Clindamycin was added in 72.3% of patients. Details are provided in Table I.
| *Unless indicated otherwise. CRP, C-reactive protein; CT, computed tomography; IQR, interquartile range; MRI, magnetic resonance imaging; SD, standard deviation; WBC, white blood cell. | |
| Table I. Demographic and clinical features of the patients. | |
| Characteristics |
|
| Age (months), mean ± SD |
|
| ≤5 years of age |
|
| >5 years of age |
|
| Sex | |
| Male |
|
| Female |
|
| Signs and symptoms | |
| Periorbital swelling |
|
| Periorbital erythema |
|
| Fever |
|
| Periorbital pain |
|
| Purulent discharge |
|
| Predisposing factors |
|
| Sinusitis |
|
| Odontogenic infection |
|
| Conjunctivitis |
|
| Insect bite |
|
| Local trauma |
|
| Laboratory findings | |
| WBC (/mm3), median (IQR) |
|
| CRP (mg/L), median (IQR) |
|
| Radiologic imaging |
|
| MRI |
|
| CT |
|
| Antibiotic therapy | |
| Any beta-lactam antibiotic |
|
| - Ampicillin-sulbactam |
|
| - Amoxicillin-clavulanate |
|
| - Ceftriaxone |
|
| - Cefotaxime |
|
| Clindamycin |
|
| Vancomycin |
|
| Metronidazole |
|
| Ciprofloxacin |
|
| Length of stay (days), median (IQR) |
|
Length of stay
Median LOS was 5 days (IQR: 3–7). No significant differences in LOS were observed by age group, sex, or presence of predisposing factors such as sinusitis or dental infections (p>0.05) (Table II). A strong positive correlation was found between LOS and total hospital cost (Spearman’s rho = 0.775, p<0.001).
| a Mann Whitney U test was used to compare two groups; IQR, interquartile range. | |||
| Table II. Comparison of length of stay by demographic and clinical characteristics. | |||
| Characteristics | Group |
|
|
| Sex | Male |
|
|
| Female |
|
||
| Age | ≤ 5 years |
|
|
| > 5 years |
|
||
| Sinusitis | Present |
|
|
| Absent |
|
||
| Odontogenic infection | Present |
|
|
| Absent |
|
||
| Conjunctivitis | Present |
|
|
| Absent |
|
||
| Insect bite | Present |
|
|
| Absent |
|
||
| Local trauma | Present |
|
|
| Absent |
|
||
| Fever | Present |
|
|
| Absent |
|
||
Hospital costs
Total hospital expenditure was 25,412.95 USD. Antibiotics accounted for the highest share (48.3%), followed by inpatient floor costs (21.9%), other medications (12.2%), laboratory tests (8.8%), and radiology (8.8%). Median per-patient cost was 123.26 USD. Patients with sinusitis or odontogenic infections had significantly higher costs (p=0.007 and p=0.030, respectively). Antibiotic and medication costs were the primary contributors to this difference.
Among the antibiotics used, the average daily vial costs were as follows: ampicillin-sulbactam 4.65 USD, amoxicillin-clavulanate 9.00 USD, ceftriaxone 4.03 USD, cefotaxime 6.07 USD, clindamycin 4.41 USD, vancomycin 7.10 USD, metronidazole 3.61 USD, and ciprofloxacin 6.17 USD.
Full data on the overall cost distribution are presented in Table III, Table IV, and Table V.
| IQR, interquartile range; USD, United States dollars. | ||
| Table III. Hospital cost distribution and per-patient costs. | ||
| Total cost (USD), n (%) | Per-patient cost, median (IQR) (USD) | |
| Inpatient floor | 5,575.03 (21.9%) | 27.74 (18.49–44.00) |
| Radiology | 2,229.84 (8.8%) | 6.07 (3.02–11.74) |
| Laboratory | 2,230.66 (8.8%) | 10.20 (6.95–16.46) |
| Antibiotics | 12,267.64 (48.3%) | 53.71 (29.81–94.59) |
| Other medications | 3,109.78 (12.2%) | 12.32 (3.27–21.34) |
| Total hospital cost | 25,412.95 (100.0%) | 123.26 (75.45–188.43) |
| a Mann Whitney U test was used to compare two groups; IQR, interquartile range; USD, United States dollars. | |||
| Table IV. Comparison of total hospital cost per patient by demographic and clinical characteristics.p valuea | |||
| Characteristics | Group | Per-Patient Cost, median (IQR) (USD) |
|
| Sex | Male | 128.72 (78.65–197.54) |
|
| Female | 115.51 (65.03–177.17) | ||
| Age | ≤ 5 years | 112.85 (75.33–156.15) |
|
| > 5 years | 138.16 (75.18–216.07) | ||
| Sinusitis | Present | 161.49 (115.19–204.06) |
|
| Absent | 113.06 (69.43–183.65) | ||
| Odontogenic infection | Present | 179.60 (96.67–209.73) |
|
| Absent | 116.87 (70.84–178.46) | ||
| Conjunctivitis | Present | 149.10 (114.13–257.70) |
|
| Absent | 118.46 (69.71–185.62) | ||
| Insect bite | Present | 76.71 (54.34–195.16) |
|
| Absent | 124.18 (80.20–189.88) | ||
| Local trauma | Present | 109.69 (63.00–149.27) |
|
| Absent | 124.07 (76.43–194.49) | ||
| Fever | Present | 132.23 (73.17–171.45) |
|
| Absent | 121.79 (75.86–201.16) | ||
| a Mann Whitney U test was used to compare two groups; IQR, interquartile range; USD, United States dollars. | |||
| Table V. Comparison of per-patient hospital costs by presence of sinusitis. | |||
| With sinusitis | Without sinusitis | p valuea | |
| Inpatient floor | 34.92 (24.62–46.19) | 25.13 (17.13–44.00) | >0.05 |
| Radiology | 10.03 (6.90–28.47) | 10.20 (6.95–16.01) | >0.05 |
| Laboratory | 8.23 (3.16–14.45) | 5.50 (3.01–10.55) | >0.05 |
| Antibiotics | 79.98 (46.61–106.82) | 49.18 (28.36–85.71) | 0.010 |
| Other medications | 17.37 (5.94–34.63) | 11.25 (3.02–19.80) | 0.030 |
| Total hospital cost | 161.49 (115.19–204.06) | 113.06 (69.43–183.65) | 0.007 |
Multivariable analysis of total hospital cost
In the multivariable generalized linear model with gamma distribution and log link function, LOS was identified as the strongest factor independently associated with total hospital cost. Each additional hospital day was associated with an approximately 15% increase in cost after adjustment for clinical and demographic variables. Age was also independently associated with higher total costs, with increasing age corresponding to a gradual rise in expenditure.
Odontogenic infection remained independently associated with higher total hospital costs, corresponding to an approximately 25% increase compared with patients without dental involvement. In contrast, sex and the presence of sinusitis were not independently associated with total hospital cost after multivariable adjustment. The results of the multivariable analysis are summarized in Table VI.
| a p values were obtained from a multivariable generalized linear model with gamma distribution and log link function; CI, confidence interval; SE, standard error. | ||||
| Table VI. Multivariable analysis of factors associated with total hospital cost. | ||||
| Variable |
|
|
|
|
| Sex (male vs female) |
|
|
|
|
| Sinusitis (present vs absent) |
|
|
|
|
| Odontogenic infection (present vs absent) |
|
|
|
|
| Age (months) |
|
|
|
|
| Length of stay (days) |
|
|
|
|
Discussion
This study evaluated 166 pediatric patients hospitalized with preseptal cellulitis. Sinusitis and odontogenic infections were identified as the leading predisposing factors in over half of the cases. While the median LOS was five days and not significantly affected by demographic or clinical factors, it strongly correlated with total hospital costs. Antibiotic treatment represented the largest portion of healthcare expenditure, particularly in patients with sinusitis or dental infections.
The clinical presentation in our cohort was consistent with previous studies, with swelling and erythema being the most prominent features.1,3,9 Due to the diagnostic overlap with orbital cellulitis and the challenges of conducting a thorough physical examination in pediatric patients, imaging was commonly employed. MRI was preferred over CT, likely reflecting concerns about radiation exposure. Imaging-related costs accounted for 8.8% of total hospitalization expenses, aligning with earlier reports from the same institution.3
Sinusitis was again identified as the most common predisposing factor and was associated with increased overall treatment costs. However, in contrast to earlier findings,3 we did not observe significant differences in imaging or laboratory expenditures between patients with and without sinusitis. This may reflect evolving clinical practices—such as more standardized imaging protocols—or changes in hospital cost structures over time. Similar findings have been reported in other studies, where sinusitis contributed to prolonged hospitalization and higher total costs, but did not specifically increase imaging or laboratory expenses.3,8 Notably, sinusitis was not independently associated with total hospital cost after multivariable adjustment, suggesting that its impact on cost may be largely mediated through other factors.
In studies on periorbital cellulitis, the most commonly isolated pathogen is Staphylococcus aureus, followed by coagulase-negative staphylococci and various Streptococcus species.7,10,11 Although the widespread use of Haemophilus influenzae type b (Hib) and pneumococcal vaccines has reduced the prevalence of these pathogens, they remain significant risk factors in incompletely vaccinated patients.7 Ampicillin-sulbactam is commonly the preferred agent for treating preseptal cellulitis associated with sinusitis or odontogenic infections.5,10 In our study, 44% of patients received either ampicillin-sulbactam or amoxicillin-clavulanate, while 56% were treated with third-generation cephalosporins. Clindamycin was added to beta-lactam antibiotic regimens in 72.3% of patients, and vancomycin was included in 4.2%. The high rate of clindamycin use (72.3%) likely reflects concerns about methicillin-resistant S. aureus (MRSA) and anaerobic coverage. Murphy et al.12 reported that in pediatric periorbital cellulitis, a combination of another anti-anaerobic drug (metronidazole) and ceftriaxone was the drug of choice for preseptal cellulitis with a rate of 73.9%. However, this pattern warrants attention, as unnecessary use of broad-spectrum antibiotics may contribute to antimicrobial resistance. Development of evidence-based treatment protocols may help reduce variation and improve cost-efficiency. Among beta-lactam antibiotics, ampicillin-sulbactam was found to be more cost-effective compared to amoxicillin-clavulanate, and ceftriaxone had a lower cost than cefotaxime.
In our study, a significant and strong correlation was found between LOS and total hospital cost. Importantly, this association remained robust after multivariable adjustment. The median LOS for our patients was found to be 5 days, which is consistent with the average LOS reported in the literature (4.5–7.7 days).3,10,13 Okay et al.1 reported that clinical improvement occurred more rapidly in children aged ≤5 years compared to those older than 5 years. Similarly, Çağlar et al.3 noted prolonged hospitalization in patients over 5 years of age and those with sinusitis. However, in our study, no significant effect of age groups and predisposing factors such as sinusitis, odontogenic infection, conjunctivitis, insect bite, and local trauma on the LOS was observed.
This study is one of the few in the literature to provide a detailed cost analysis related to healthcare utilization in pediatric patients hospitalized with a diagnosis of preseptal cellulitis. Furthermore, it makes a significant contribution due to its larger sample size and reflection of current data compared to previous studies. However, the main limitation of our study is its single-center and retrospective design. Data collection through patient records may lead to information gaps such as incomplete documentation of some clinical findings. The lack of a standardized protocol in examination and treatment processes is another important factor that may affect cost analysis. Similarly, the relatively high utilization of radiologic imaging might have contributed to an increase in total hospital costs.
In conclusion, our findings reveal that antibiotic expenses constitute the largest component of costs in pediatric patients hospitalized with a diagnosis of preseptal cellulitis. Furthermore, the presence of sinusitis and odontogenic infections was identified as a contributing factor to increased overall costs. Radiologic imaging also represents a considerable component of total hospital costs; its rational limitation, when clinically appropriate, may help reduce both overall expenses and unnecessary radiation exposure. LOS and odontogenic infection were identified as independent drivers of increased total cost, highlighting potential targets for cost containment through optimized discharge planning and focused management of dental-source infections. The implementation of standardized treatment protocols and the promotion of rational antibiotic use may play a crucial role in optimizing healthcare resource utilization and preventing antibiotic resistance.
Ethical approval
The study was approved by ethics committee of Dr. Behçet Uz Children’s Hospital (date: March 06, 2025, number: 2025/05-09).
Source of funding
The authors declare the study received no funding.
Conflict of interest
The authors declare that there is no conflict of interest.
References
- Okay B, Kalinbacoglu CD, Akkoc G, et al. Evaluating hospitalized children for preseptal cellulitis: a single-center experience and current literature review. North Clin Istanb 2025; 12: 89-94. https://doi.org/10.14744/nci.2023.58630
- Ekhlassi T, Becker N. Preseptal and orbital cellulitis. Dis Mon 2017; 63: 30-32. https://doi.org/10.1016/j.disamonth.2016.09.002
- Çağlar İ, Kafes C, Korcum M, et al. Hospital cost analysis of children with preseptal cellulitis. Int J Pediatr Otorhinolaryngol 2018; 106: 96-99. https://doi.org/10.1016/j.ijporl.2018.01.007
- Buchanan MA, Muen W, Heinz P. Management of periorbital and orbital cellulitis. Paediatr Child Health 2012; 22: 72-77. https://doi.org/10.1016/j.paed.2011.12.002
- Cooper BJ, Mitchell ML, Melamed S, Liegl M, Pan AY, Burek AG. Improving antibiotic use in pediatric preseptal cellulitis using a clinical practice guideline. Hosp Pediatr 2024; 14: 791-798. https://doi.org/10.1542/hpeds.2023-007581
- Georgakopoulos CD, Eliopoulou MI, Stasinos S, Exarchou A, Pharmakakis N, Varvarigou A. Periorbital and orbital cellulitis: a 10-year review of hospitalized children. Eur J Ophthalmol 2010; 20: 1066-1072. https://doi.org/10.1177/112067211002000607
- Shehada W, Onyejesi CD, Ram MD, et al. Periorbital and orbital cellulitis in pediatric emergency medicine: diagnostic challenges and evidence-based guidance. Curr Treat Options Peds 2025; 11: 12. https://doi.org/10.1007/s40746-025-00327-7
- Padia R, Thomas A, Alt J, Gale C, Meier JD. Hospital cost of pediatric patients with complicated acute sinusitis. Int J Pediatr Otorhinolaryngol 2016; 80: 17-20. https://doi.org/10.1016/j.ijporl.2015.11.021
- Santos JC, Pinto S, Ferreira S, Maia C, Alves S, da Silva V. Pediatric preseptal and orbital cellulitis: a 10-year experience. Int J Pediatr Otorhinolaryngol 2019; 120: 82-88. https://doi.org/10.1016/j.ijporl.2019.02.003
- Devrim I, Kanra G, Kara A, et al. Preseptal and orbital cellulitis: 15-year experience with sulbactam ampicillin treatment. Turk J Pediatr 2008; 50: 214-218.
- Shih EJ, Chen JK, Tsai PJ, Lin MC, Bee YS. Antibiotic choices for pediatric periorbital cellulitis-a 20-year retrospective study from Taiwan. Antibiotics (Basel) 2022; 11: 1288. https://doi.org/10.3390/antibiotics11101288
- Murphy DC, Meghji S, Alfiky M, Bath AP. Paediatric periorbital cellulitis: a 10-year retrospective case series review. J Paediatr Child Health 2021; 57: 227-233. https://doi.org/10.1111/jpc.15179
- Gonçalves R, Menezes C, Machado R, Ribeiro I, Lemos JA. Periorbital cellulitis in children: analysis of outcome of intravenous antibiotic therapy. Orbit 2016; 35: 175-180. https://doi.org/10.1080/01676830.2016.1176205
Copyright and license
Copyright © 2026 The Author(s). This is an open access article distributed under the Creative Commons Attribution License (CC BY), which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is properly cited.









