Abstract
Globally, an estimated 12-13% of children experience sexual abuse, with prevalence rates of approximately 18% among girls and 8% among boys. Clinicians evaluating pediatric patients who present with anogenital complaints or lesions face considerable diagnostic challenges. The purpose of this narrative review is to outline the most frequently encountered conditions that can mimic child sexual abuse (CSA), thereby raising clinical awareness and helping to minimize both false-positive and false-negative diagnoses. We conducted a semi-systematic literature search in PubMed covering the period from 2000 to 2025, using the search terms “child sexual abuse,” “differential diagnosis,” “mimics,” and “mimickers,” supplemented by the German interdisciplinary guideline on child abuse and neglect. Notably, the vast majority of children who have been sexually abused present without detectable physical abnormalities. Conversely, an erroneous diagnosis of abuse—or the failure to identify a treatable underlying condition—can carry severe consequences. Many practitioners in primary care lack sufficient training to distinguish the wide range of dermatologic and systemic disorders that may affect the anogenital region. Precise recognition, careful documentation, and scientifically grounded interpretation of physical findings are critical to ensue child protection. Optimal medical care for suspected CSA victims requires that clinicians possess expertise in pediatric and adolescent gynecology and forensic medicine, recognize the constraints inherent to physical examination findings, and consistently employ up-to-date classification frameworks and clinical guidelines. Heightened awareness of CSA mimickers is essential both to prevent unfounded allegations and to ensure timely, appropriate management of genuine abuse.
Keywords: child sexual abuse, differential diagnosis, mimickers, accidental anogenital injury, cutaneous lesions
Introduction
Child sexual abuse (CSA) constitutes a pervasive public health concern, with meta-analytic data indicating that 12-13% of children worldwide are affected—roughly 18% of girls and 8% of boys.1 These figures, however, almost certainly underestimate the true scope of the problem, as a substantial proportion of cases remain undisclosed. Robust epidemiological data and standardized frameworks for addressing the medical and legal dimensions of CSA are still evolving.
CSA encompasses a spectrum of sexual activities imposed on children and adolescents who, by virtue of their developmental stage, are unable to provide informed consent or participate as equal partners.2,3 Such acts transgress societal norms and are characterized by an inherent power asymmetry, whereby offending adults leverage age-related authority—through psychological manipulation, coercion, or physical force—to gratify their own sexual interests. The range of abusive behaviors extends from non-contact offenses (e.g., exposure, voyeurism) to penetrative assault. In most instances, CSA is a recurring and profoundly traumatizing experience, frequently perpetrated by family members or other individuals occupying positions of trust.3,4 Victims commonly develop intense feelings of guilt, shame, diminished self-worth, and social withdrawal, with well-documented long-term repercussions for mental, emotional, and physical health.4
Given its high prevalence and far-reaching sequelae, CSA has attracted growing attention in both medical practice and the criminal justice system.5 Media coverage regularly highlights cases of child victimization, yet professional awareness often becomes acute only in the aftermath of individual tragedies. Research consistently shows that many clinicians who encounter pediatric patients have insufficient training in recognizing, diagnosing, and managing CSA.6 Diagnostic errors persist despite advances in the field, and conditions that mimic the presentation of sexual abuse remain poorly understood by many practitioners. Anogenital complaints in children demand careful clinical evaluation, as both failures to identify genuine abuse and a false attribution of abuse to an innocent cause can have devastating consequences. Accordingly, healthcare providers must be well versed in the differential diagnosis of CSA, due to the subsequent health of the victim and to the possible criminal consequences.
The aim of this review is to provide a comprehensive overview of the conditions most commonly mistaken for CSA, with the dual objective of reducing erroneous diagnoses and improving timely recognition of sexual abuse.
Because unexplained skin changes in the anogenital region are among the most frequent initial presentations that prompt suspicion of CSA, accurate differentiation of cutaneous mimickers from genuine abuse-related findings is of paramount importance.7 Misidentification in either direction carries serious implications for the child, the family, and any individual wrongly accused.
By synthesizing the available evidence on CSA mimickers, we intend to equip clinicians across specialties with the knowledge needed to navigate these diagnostically challenging presentations and to reduce the burden of false accusations while strengthening the identification of true CSA.
Methods
We performed a semi-systematic review of the literature published between January 2000 and December 2024. PubMed was searched using the following terms in various combinations: “child sexual abuse,” “differential diagnosis,” “mimics,” and “mimickers.” In addition, the German interdisciplinary guideline on child abuse and neglect (S3-Leitlinie Kindesmisshandlung, -missbrauch, -vernachlässigung) was consulted. The initial search yielded 58 publications, of which 39 met our predefined inclusion criteria: (i) peer-reviewed original research addressing conditions that mimic CSA, (ii) pediatric study population (age <18 years), (iii) English-language publication, and (iv) publication date within the specified timeframe. We excluded practice guidelines, commentaries, editorials, opinion pieces, and studies focusing primarily on adult populations or published in languages other than English. Several limitations of the available evidence warrant acknowledgment. The heterogeneity of study designs and outcome measures precluded formal meta-analysis, and many included studies were case reports or small case series, limiting generalizability. Nevertheless, the growing recognition that CSA requires a multidisciplinary approach—integrating clinical, forensic, and psychosocial perspectives—underscores the importance of consolidating the existing knowledge base. Further research is needed to enhance the competency of healthcare professionals, particularly those with forensic responsibilities, in the differential diagnosis of CSA.
Anogenital findings in abused children
The spectrum of anogenital findings following CSA is broad and depends on multiple factors, including the nature and chronicity of the abuse, any objects used, the degree of force applied, the victim’s age, and the extent of resistance.8 Among the variables most strongly associated with identifiable findings are the child’s report of pain, the presence of vaginal bleeding, and the interval between the most recent abusive episode and the medical examination. Structured classification systems play a central role in the standardized assessment and interpretation of such findings. The Adams classification, which stratifies findings into three tiers, has gained wide acceptance as the principal framework for evaluating anogenital examination results in cases of suspected CSA. This system has undergone iterative, consensus-driven revision, with the most recent update published in 2023 (Table I).9 Within this scheme, findings are categorized as those suggestive of abuse and those considered specific for abuse (Table II).9,10
| CSA: child sexual abuse. | |
| Table I. Simplified version of the Adam`s classification. | |
| Adams I | Normal findings or findings with a medical explanation other than abuse |
| Adams II | Findings of unclear significance that arouse the suspicion of CSA |
| Adams III | Findings of injury that establish the diagnosis of CSA |
| Table II. Anogenital findings specific for abuse. | |
| Moderate specificity for abuse | High specificity for abuse |
|
|
Physiological anogenital findings
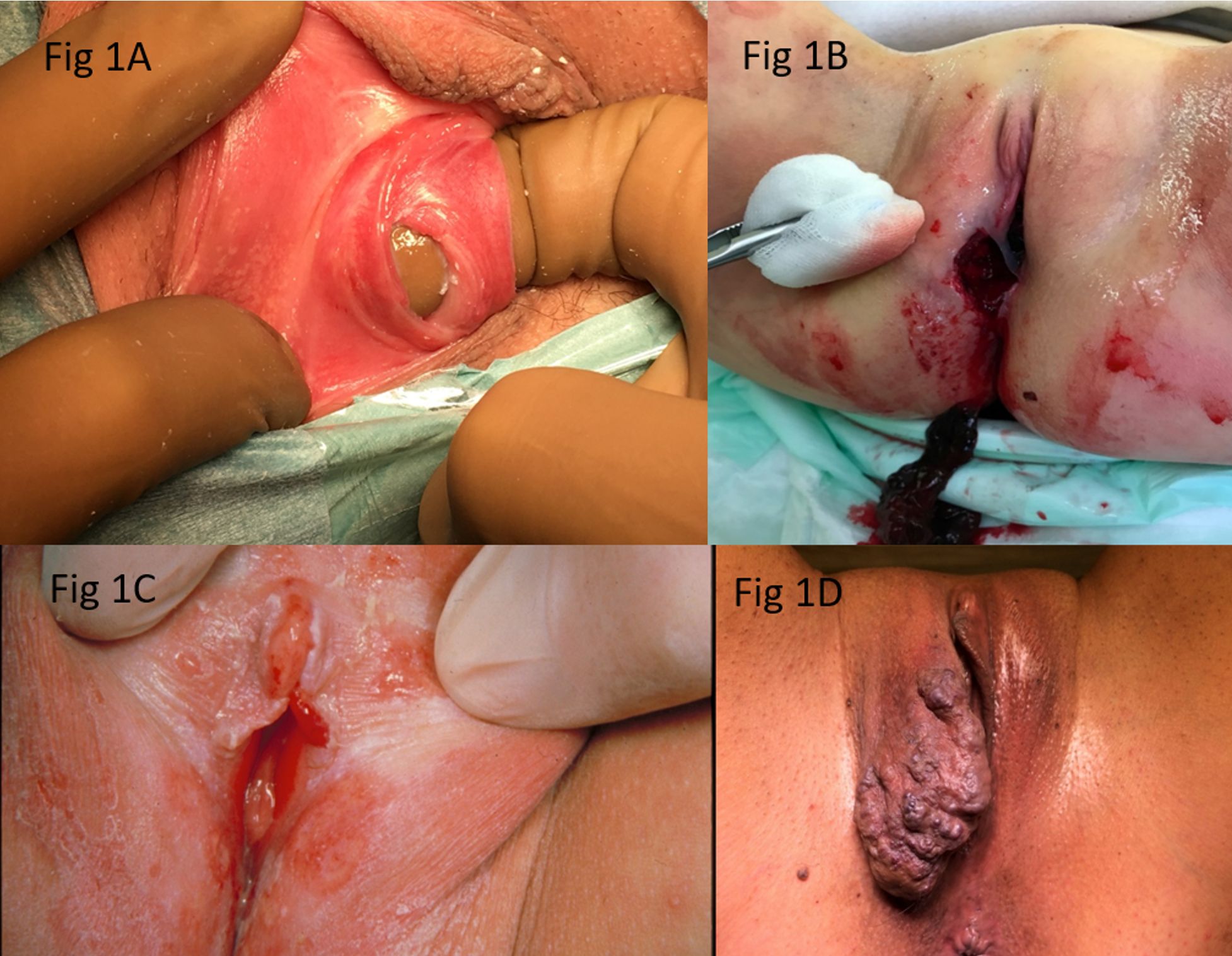
The morphology of the external genitalia, and particularly of the hymen, varies with age, constitutional factors, and hormonal status. Recognized hymenal configurations include semilunar, cribriform, septate, and imperforate variants. External hymenal ridges—thin, symmetric fibrous bands located lateral to the urethra that reinforce the superior hymenal margin—may be mistaken for scarring from prior trauma. These peri-urethral supporting ligaments typically course toward the lateral vaginal wall and are of no pathological significance.3,11 Additional physiological variants include congenital absence of the superior hymenal rim, hymenal septa (Fig. 1A), protrusions, indentations, and punctuations of the inferior hymenal margin.3,11 Longitudinal intravaginal ridges that traverse the vaginal columns may protrude and alter the contour of the hymenal opening, representing yet another normal anatomical variation best appreciated during examination in the knee-chest position. Certain structures in the vestibular and perineal region may closely resemble healed injuries. The linea vestibularis—an avascular, midline linear structure extending from the inferior hymen to the posterior fourchette—can be confused with a healed laceration.12 Similarly, failure of midline fusion, which extends from the fourchette along the perineum toward the anus, may mimic a fresh wound. Perianal skin tags, particularly when located in the midline, are another normal variant; lateral displacement of such tags, however, may warrant further evaluation for possible CSA.13 A summary of physiological genital and anal findings in children is provided in Table III.3,9 Importantly, a number of examination findings formerly interpreted as indicators of abuse are now understood to represent normal anatomical variation. Measurement of hymenal opening diameter, for example, is considered obsolete and of no diagnostic utility. Tampon use may widen the hymenal orifice in pubertal girls without causing tissue injury, and activities such as horseback riding, gymnastics, stretching, and masturbation have not been shown to produce hymenal damage.
| Table III. Physiological genital and anal findings. | |
|
|
|
| Genital findings in girls | Anal findings |
| Various hymenal configurations: septate, semilunar, microperforate, cribriform, imperforate | Perianal erythema |
| External hymenal ridges | Perianal pigmentation |
| Longitudinal intravaginal ridges | Circular venous engorgement |
| Hymeneal tags | Perianal polyp-like tags |
| Periurethral bands | Diastasis ani |
| Erythema in introitus | Perianal erythema |
| Congenital pigmentation | |
| Urethral dilatation | |
Accidental anogenital injury
Accidental trauma to the anogenital region is one of the more frequently encountered differential diagnoses.14 Such injuries are a source of considerable alarm for both caregivers and clinicians, who must determine whether the mechanism was unintentional or inflicted and, in the latter case, whether a report to child protective services is indicated. The hypoestrogenic state of the prepubertal genitalia predisposes to more profuse bleeding than might otherwise be expected.15 Genital trauma in prepubertal children—particularly when the hymen is involved—invariably raises the question of sexual abuse. Distinguishing accidental from inflicted injury depends critically on the concordance between the reported mechanism and the observed pattern of trauma. Straddle injuries, in which the perineum strikes an object during a fall, are a common form of accidental genital trauma with a characteristic presentation that rarely involves the hymen. An example of such an injury is illustrated in Fig. 1B. When hymenal trauma is present, suggesting possible penetrating injury, the clinician must consider the potential for significant intravaginal or intra-abdominal visceral injury, which may occasionally present with deceptively mild symptoms.16 Published reports of accidental anogenital trauma, while limited in number, consistently emphasize the critical role of a detailed, internally consistent history in formulating the differential diagnosis. Fortunately, genital and anal injuries requiring operative intervention are uncommon in prepubertal girls; in one series of 358 girls aged 0-16 years with blunt perineal trauma, only 9% required surgical repair.17 Anorectal injuries in children are similarly uncommon and are most often attributed to falls during play or, alternatively, to CSA. Mechanistically, straddle injuries produce crush-type trauma from falls onto objects of varying shape, typically resulting in unilateral involvement of the labia and clitoral hood. Impalement injuries, by contrast, involve penetration by a pointed object.16 Whenever hymenal injury is identified, the possibility of deeper vaginal or intraperitoneal penetration must be excluded; evaluation may include vaginoscopy, hysteroscopy, laparoscopy, or sigmoidoscopy under anesthesia, supplemented by transrectal ultrasonography or abdominal computed tomography as clinically indicated. Among inline skating injuries, the upper extremities are involved in 50% to 86% of cases, with nearly half being fractures; pelvic or pubic injuries constitute only a small minority.18 The distinguishing features of accidental versus inflicted anogenital injury are summarized in Table IV. Published reports consistently describe accidental genital injuries as predominantly minor, superficial, anterior, external, and unilateral. In the vast majority of accidental cases, the hymen remains uninjured; penetrating injuries of accidental origin are exceedingly rare.
| Table IV. Accidental anogenital injuries vs child sexual abuse. | ||
| Suggestive of accidental injury | Suggestive of sexual abuse | |
| Anatomical localisation | Anterior, exterior | Deep |
| Unilateral | Bilateral | |
| External Labia, Clitoris | External genitalia, Hymen | |
| Characteristics | Superficial | Deep |
| Mild | Serious | |
| Form of Appearance | Bruises, hematomas | Tears, penetration |
| Invasiveness | Very rare | Common |
| Penetration | Very rare | Common |
| History | Acute, dramatic, consistent | Chronic, not consistent |
| Medical care | Acute, emergency | not acute, rare |
Cutaneous mimickers of child sexual abuse
A variety of dermatologic conditions may produce anogenital findings that simulate CSA. Among the most important is lichen sclerosus (LS), a chronic autoimmune inflammatory dermatosis that causes epithelial atrophy, hypopigmentation, and—in some cases—prominent subcutaneous hemorrhage in the perivaginal and perianal region, creating the characteristic “hourglass” appearance (Fig. 1C). Approximately 95% of patients with LS develop genital lesions, whereas extragenital involvement occurs in only 6-15% of cases. The hymen itself is characteristically spared.19,20 The haemorrhagic changes, fissuring, and ulceration associated with LS can closely resemble the sequelae of sexual abuse. Although the condition predominantly affects postmenopausal women (with a 90% female preponderance overall), approximately 15% of cases occur in childhood. Extragenital lesions, when present, tend to involve the upper trunk, forearms, neck, and face. Patients typically report genital pruritus, pain, and bleeding; in chronic cases, labial fusion in girls or phimosis in boys may develop. The diagnosis is based on the clinical presentation and can be confirmed by targeted biopsy. While no curative therapy exists, topical corticosteroids provide significant symptomatic relief. When initially assessed by a multidisciplinary team including forensic specialists, the clinical picture can usually be distinguished from traumatic injury, and the diagnosis of LS established by routine methods. Despite its recognizable features, LS has been misdiagnosed not only as CSA but also as gonococcal vaginitis, lichen planus, psoriasis, and self-inflicted injury.21 Several additional conditions merit consideration in the differential diagnosis of cutaneous CSA mimickers. Congenital dermal melanocytosis, phytophotodermatitis, and certain connective tissue disorders may all be erroneously attributed to abuse.18 Infantile hemangiomas—the most common tumors of infancy, occurring with greater frequency in girls and premature infants—may present on cutaneous or mucosal surfaces within the first weeks of life.20 Although the majority involute spontaneously, complications (most commonly ulceration, occurring in approximately 5% of cases) can occur.22 Hemangiomas are classified as superficial (bright red, lobulated), deep (bluish subcutaneous masses), or mixed. When located in the perineal region, their red coloration and propensity for ulceration can be mistaken for abuse-related findings (Fig. 1D). Allergic contact dermatitis (ACD) is an additional diagnostic pitfall. This delayed-type hypersensitivity reaction produces well-demarcated, pruritic, eczematous plaques—with or without vesiculation—at sites of allergen exposure. In the genital area, common triggers include detergents, hygiene products, and nickel. The clinical history and distribution pattern typically suffice for diagnosis. Isolated case reports of ACD in the anogenital region being misinterpreted as CSA have been published.23,24
Vaginal and perianal infections mistaken as CSA
Vulvovaginitis is among the most common gynecologic complaints in prepubertal girls, attributable to several predisposing factors: the relatively small labia offer limited mechanical protection, the hypoestrogenic mucosa is thin and atrophic, and the neutral intravaginal pH favours pathogen colonization. Inadequate hygiene further promotes chronic irritation and secondary bacterial infection. Commonly implicated organisms include Staphylococcus aureus, group A β-haemolytic Streptococcus, Enterococcus, and Shigella species. Streptococcal vulvovaginitis and perianal streptococcal cellulitis are particularly notable presentations; the latter typically manifests with painful defecation and constipation, occurs more frequently in boys, and is usually unaccompanied by systemic symptoms. In girls, vulvovaginitis may present with vaginal discharge, pruritus, and erythema. The clinical appearance of both conditions can prompt erroneous suspicion of CSA.7 Anogenital warts (AGW) represent another challenging differential diagnosis. These papillomatous growths, caused predominantly by human papillomavirus (HPV) types 6, 11, 16, and 18, may be acquired through perinatal transmission, auto- or heteroinoculation (e.g., from hands or during diaper changes), or direct contact with symptomatic or asymptomatic HPV carriers. Perinatal acquisition is generally considered unlikely beyond the age of two years25, although vertical transmission may explain lesions detected in infants under one year.26 Non-sexual transmission routes—including shared bathing and towel use—have also been documented.9 The warts are typically soft, small (<1 mm), and frequently asymptomatic, though pruritus may occur. While the presence of AGW in a child does not constitute definitive evidence of CSA, the possibility of abuse cannot be excluded regardless of the child’s age, and alternative transmission routes should be actively explored.27 Additional differential diagnoses of vulvovaginal vesicular lesions include herpes zoster and Epstein-Barr virus infection.28
Labial adhesion (also termed labial agglutination) describes partial or complete fusion of the labia minora or, less commonly, the labia majora, most often occurring posteriorly along the midline. The pathogenesis is not fully elucidated but is thought to involve hypoestrogenism and local inflammation. Topical estrogen cream is the first-line treatment for symptomatic cases; following pretreatment, gentle manual separation is often successful. The condition is most prevalent between the ages of one and three years; when observed in older children, the possibility of CSA should be considered.8
Vaginal bleeding in prepubertal girls is most frequently attributable to infection (approximately 70% of cases), with less common etiologies including foreign bodies, hemangiomas, and precocious puberty.3 Intravaginal foreign bodies constitute a particular diagnostic challenge in pediatric gynecology; the most commonly identified foreign body is retained toilet paper, typically presenting with persistent malodorous discharge. Only 10% of affected patients initially present with the specific complaint of a possible foreign object. Ultrasonography demonstrates superior sensitivity (approximately 80%) compared with plain radiography (approximately 33%) for foreign body detection.29 Vaginoscopy remains the diagnostic and therapeutic gold standard and is additionally required to exclude sarcoma botryoides.
Among the principal differential diagnoses of perianal findings suggestive of abuse are anal fissures secondary to chronic constipation or Crohn disease, rectal prolapse, and proctitis (e.g., due to cytomegalovirus infection).3 Crohn disease, a chronic inflammatory bowel disorder with potential involvement of any segment of the gastrointestinal tract, frequently produces perianal fissures, fistulae, and skin tags that may raise suspicion of CSA.30 Documented cases of Crohn disease initially misdiagnosed as CSA underscore the importance of considering this entity in the differential.31
Urogenital pathologies
Urethral pathologies—including hemangiomas, polyp-like tags, ureteroceles, and urethral prolapse—are infrequently encountered in pediatric practice and are consequently prone to misdiagnosis.32 Urethral prolapse (UP) occurs predominantly in prepubertal girls between four and eight years of age, with a predilection for children of African descent. Contributing factors include increased intra-abdominal pressure (as in chronic constipation or persistent coughing) and hypoestrogenism. The most common presenting symptom is bleeding (reported in approximately 86% of cases), followed by a visible mass at the introitus (47%) and dysuria (32%).33 Dysuria itself is a frequent complaint associated with genital trauma of any cause, but it must also be differentiated from excessive self-stimulatory behaviour, exposure to genital irritants, and CSA.
Discussion
Pooled data from 39 prevalence studies spanning 28 countries and the period 1994-2007 indicate that 10-20% of girls and 5-10% of boys experience CSA, findings that are broadly concordant with earlier estimates.34 A large-scale meta-analysis encompassing 323 studies and 9.9 million affected children calculated a global prevalence of 12.7%, with rates of 18.0% for girls and 7.6% for boys.1 It has been noted that “Child sexual abuse is more common than childhood cancer, juvenile diabetes, and congenital heart disease combined…”.35 Nonetheless, an estimated 95% of cases are never reported to authorities.36 Data from Germany remain particularly scarce, and reliable information on the frequency of specific abuse subtypes is limited. A substantial body of evidence links childhood sexual victimization to chronic mental and physical illness in adulthood.2,3,9 Evidence-based research and consensus-driven clinical standards in this domain have gained traction in Germany and internationally only in recent years.3
The evaluation of a child with suspected CSA demands time, specialized training, and unwavering professional commitment. Clinicians must balance empathy with scientific rigor—an approach aptly described as “cool science for a hot topic.” Although more than 90% of abused children present with unremarkable physical examination findings9,35,37, the forensic component of the assessment remains indispensable: the absence of positive findings can itself be forensically significant. The objectives of the medical examination include corroborating or refuting the suspicion of abuse, providing acute care, screening for sexually transmitted infections, assessing for pregnancy and administering emergency contraception where appropriate, offering timely reassurance to the child and family, and collecting and documenting evidence for potential legal proceedings. In most cases, the diagnosis rests primarily on the child’s disclosure, obtained through empathetic, non-leading questioning by a trained interviewer.3 Suggestive or leading questions must be strictly avoided, and the child’s statements should be recorded verbatim by professionals experienced in forensic interviewing. The physical examination, when conducted in a supportive and non-coercive manner, can have a therapeutic effect by affirming the child’s bodily integrity. Where indicated, prophylaxis against sexually transmitted infections or pregnancy may be initiated. In Germany, the Bundeskinderschutzgesetz (Federal Child Protection Act) delineates the circumstances under which a physician may breach confidentiality to report relevant information to the Youth Welfare Office.
The differential diagnostic workup of suspected CSA presents a formidable challenge for healthcare professionals, pediatric and adolescent gynecologists, and forensic practitioners. Clinicians must be prepared to distinguish accidental or self-inflicted injuries and medical conditions that mimic maltreatment from genuine abuse. This process requires meticulous evaluation, adequate time, and subspecialty expertise spanning both pediatric gynecology and forensic medicine. The examiner must be conversant with the current evidence regarding the medical findings of CSA and their classification.38 Given that normal examination findings are documented in 90-95% of evaluated cases, physical findings alone only rarely yield a definitive diagnosis. Indeed, only an estimated 5% of CSA cases are accompanied by examination findings that are independently diagnostic. The most commonly observed genital injuries are superficial and typically heal before the abuse is disclosed or concern is raised.
Conclusions
The majority of primary care practitioners receive insufficient training in the recognition of dermatologic and systemic conditions affecting the anogenital region, while dermatologists may not routinely consider the possibility of sexual abuse in their differential. Accurate identification of CSA is of equal importance to the avoidance of false accusations, and the medical assessment constitutes only one component of a comprehensive, multidisciplinary evaluation. The consequences of diagnostic error, whether over- or under-diagnosis, extend to the child, the family, and any individual wrongly implicated. It is therefore imperative that all healthcare providers involved in pediatric care, particularly gynecologists and pediatricians, maintain a thorough awareness of conditions that mimic CSA. Careful attention to clinical clues such as congenital onset and a family history of similar dermatoses can be highly informative. Expert examination under optimal conditions, performed by a clinician familiar with the full spectrum of potential mimickers, is essential for reaching the correct diagnosis. Whenever diagnostic uncertainty persists, referral to a dermatologist should be pursued to exclude genuine skin disease. Healthcare professionals should be encouraged to report and publish cases in which non-abusive conditions were initially mistaken for CSA, thereby expanding the collective knowledge base and fostering greater diagnostic accuracy. The management of these diagnostically complex presentations demands forensic expertise, subspecialty clinical skill, and the involvement of a coordinated multidisciplinary team. Clinicians must also remain alert to the possibility that genuine abuse and coexisting medical conditions may occur simultaneously within the same patient.
Source of funding
The authors declare the study received no funding.
Conflict of interest
The authors declare that there is no conflict of interest.
References
- Stoltenborgh M, van Ijzendoorn MH, Euser EM, Bakermans-Kranenburg MJ. A global perspective on child sexual abuse: meta-analysis of prevalence around the world. Child Maltreat 2011; 16: 79-101. https://doi.org/10.1177/1077559511403920
- Humphreys KL, LeMoult J, Wear JG, Piersiak HA, Lee A, Gotlib IH. Child maltreatment and depression: a meta-analysis of studies using the Childhood Trauma Questionnaire. Child Abuse Negl 2020; 102: 104361. https://doi.org/10.1016/j.chiabu.2020.104361
- Herrmann B, Banaschak S, Csorba R, Navratil F, Dettmeyer R. Physical examination in child sexual abuse-approaches and current evidence. Dtsch Arztebl Int 2014; 111: 692-703. https://doi.org/10.3238/arztebl.2014.0692
- Alyce S, Taggart D, Turton J. Trust, entrusting and the role of trustworthiness for adult survivors of child sexual abuse. J Ment Health 2025; 34: 263-272. https://doi.org/10.1080/09638237.2024.2390366
- Letourneau EJ, Brown DS, Fang X, Hassan A, Mercy JA. The economic burden of child sexual abuse in the United States. Child Abuse Negl 2018; 79: 413-422. https://doi.org/10.1016/j.chiabu.2018.02.020
- Enyedy A, Csorba R. Female child sexual abuse. Orv Hetil 2017; 158: 910-917. https://doi.org/10.1556/650.2017.30771
- Reingold RE, O’Hara MA, Levin LE. Skin lesions on sensitive sites: mimickers of sexual abuse in children. Pediatr Rev 2022; 43: e15-e19. https://doi.org/10.1542/pir.2020-004317
- Csorba R, Lampé R, Póka R. Surgical repair of blunt force penetrating anogenital trauma in an 18-month-old sexually abused girl: a case report. Eur J Obstet Gynecol Reprod Biol 2010; 153: 231. https://doi.org/10.1016/j.ejogrb.2010.07.035
- Kellogg ND, Farst KJ, Adams JA. Interpretation of medical findings in suspected child sexual abuse: an update for 2023. Child Abuse Negl 2023; 145: 106283. https://doi.org/10.1016/j.chiabu.2023.106283
- Lahoti SL, McClain N, Girardet R, McNeese M, Cheung K. Evaluating the child for sexual abuse. Am Fam Physician 2001; 63: 883-892.
- Pillai M. Genital findings in prepubertal girls: what can be concluded from an examination? J Pediatr Adolesc Gynecol 2008; 21: 177-185. https://doi.org/10.1016/j.jpag.2007.08.005
- Adams JA. Understanding medical findings in child sexual abuse: an update for 2018. Acad Forensic Pathol 2018; 8: 924-937. https://doi.org/10.1177/1925362118821491
- Hornor G. A normal ano-genital exam: sexual abuse or not? J Pediatr Health Care 2010; 24: 145-151. https://doi.org/10.1016/j.pedhc.2008.10.007
- Arthur LT. Navigating the complex terrain of childhood sexual assault allegations: mimics of sexual assault in the paediatric population. J Forensic Leg Med 2025; 113: 102880. https://doi.org/10.1016/j.jflm.2025.102880
- Iqbal CW, Jrebi NY, Zielinski MD, et al. Patterns of accidental genital trauma in young girls and indications for operative management. J Pediatr Surg 2010; 45: 930-933. https://doi.org/10.1016/j.jpedsurg.2010.02.024
- Csorba R, Engel JB, Wieg C. Surgical repair of an impalement genital injury from an inline skating accident in a 7-year-old prepubertal girl: a case report. J Pediatr Adolesc Gynecol 2017; 30: e11-e13. https://doi.org/10.1016/j.jpag.2016.08.014
- McLaughlin CJ, Martin KL. Mechanism of injury and age predict operative intervention in pediatric perineal injury. Pediatr Emerg Care 2023; 39: 230-235. https://doi.org/10.1097/PEC.0000000000002928
- Osberg JS, Schneps SE, Di Scala C, Li G. Skateboarding: more dangerous than roller skating or in-line skating. Arch Pediatr Adolesc Med 1998; 152: 985-991. https://doi.org/10.1001/archpedi.152.10.985
- Abder-Rahman H, Habash I, Hussein A, Al-Shaeb A, Elqasass A, Qaqish LN. Genital lichen sclerosus misdiagnosis: forensic insights. Forensic Sci Med Pathol 2024; 20: 1444-1447. https://doi.org/10.1007/s12024-024-00779-7
- Asati DP, Singh S, Sharma VK, Tiwari S. Dermatoses misdiagnosed as deliberate injuries. Med Sci Law 2012; 52: 198-204. https://doi.org/10.1258/msl.2012.011054
- Navarro-Crummenauer B, Pickhardt CP, Urban R. Lichen sclerosus mistaken for sexual abuse-prevention of victimization. Klin Padiatr 2015; 227: 239-242. https://doi.org/10.1055/s-0034-1395616
- Cebesoy FB, Kutlar I, Aydin A. A rare mass formation of the vulva: giant cavernous hemangioma. J Low Genit Tract Dis 2008; 12: 35-37. https://doi.org/10.1097/LGT.0b013e3181255e85
- DiBianco JM, Morley C, Al-Omar O. Nocturnal enuresis: a topic review and institution experience. Avicenna J Med 2014; 4: 77-86. https://doi.org/10.4103/2231-0770.140641
- Litvinov IV, Sugathan P, Cohen BA. Recognizing and treating toilet-seat contact dermatitis in children. Pediatrics 2010; 125: e419-e422. https://doi.org/10.1542/peds.2009-2430
- Rogstad KE, Wilkinson D, Robinson A. Sexually transmitted infections in children as a marker of child sexual abuse and direction of future research. Curr Opin Infect Dis 2016; 29: 41-44. https://doi.org/10.1097/QCO.0000000000000233
- Qin X, Melvin AJ. Laboratory diagnosis of sexually transmitted infections in cases of suspected child sexual abuse. J Clin Microbiol 2020; 58: e01433-e01419. https://doi.org/10.1128/JCM.01433-19
- Jayasinghe Y, Garland SM. Genital warts in children: what do they mean? Arch Dis Child 2006; 91: 696-700. https://doi.org/10.1136/adc.2005.092080
- Garden AS. Vulvovaginitis and other common childhood gynaecological conditions. Arch Dis Child Educ Pract Ed 2011; 96: 73-78. https://doi.org/10.1136/adc.2009.181883
- Umans E, Boogaerts M, Vergauwe B, Verest A, Van Calenbergh S. Vaginal foreign body in the pediatric patient: a systematic review. Eur J Obstet Gynecol Reprod Biol 2024; 297: 153-158. https://doi.org/10.1016/j.ejogrb.2024.04.019
- Bouzidi H, Chakiri R, Amraoui N, et al. Crohn’s disease presenting as vulvar edema in a 15-year-old girl. J Dermatol Case Rep 2014; 8: 75-77. https://doi.org/10.3315/jdcr.2014.1180
- McKay GE, Liu L, Shaw KS, et al. Pediatric cutaneous Crohn disease: a case series of 89 patients and review. Pediatr Dermatol 2024; 41: 807-813. https://doi.org/10.1111/pde.15689
- Ninomiya T, Koga H. Clinical characteristics of urethral prolapse in Japanese children. Pediatr Int 2017; 59: 578-582. https://doi.org/10.1111/ped.13226
- Schaul M, Schwark T. Rare (uro-)genital pathologies in young girls mimicking sexual abuse. Int J Legal Med 2022; 136: 623-627. https://doi.org/10.1007/s00414-021-02621-z
- Pereda N, Guilera G, Forns M, Gómez-Benito J. The international epidemiology of child sexual abuse: a continuation of Finkelhor (1994). Child Abuse Negl 2009; 33: 331-342. https://doi.org/10.1016/j.chiabu.2008.07.007
- Adams JA, Farst KJ, Kellogg ND. Interpretation of medical findings in suspected child sexual abuse: an update for 2018. J Pediatr Adolesc Gynecol 2018; 31: 225-231. https://doi.org/10.1016/j.jpag.2017.12.011
- Martin EK, Silverstone PH. How much child sexual abuse is “below the surface,” and can we help adults identify it early? Front Psychiatry 2013; 4: 58. https://doi.org/10.3389/fpsyt.2013.00058
- Crawford-Jakubiak JE, Alderman EM, Leventhal JM, Committee on Child Abuse and Neglect; Committee on Adolescence. Care of the adolescent after an acute sexual assault. Pediatrics 2017; 139: e20164243. https://doi.org/10.1542/peds.2016-4243
- Focardi M, Gori V, Romanelli M, et al. “Mimics” of injuries from child abuse: case series and review of the literature. Children (Basel) 2024; 11: 1103. https://doi.org/10.3390/children11091103
Copyright and license
Copyright © 2026 The Author(s). This is an open access article distributed under the Creative Commons Attribution License (CC BY), which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is properly cited.