
Abstract
Background. Ocular involvement in the diagnosis of leukemia is clinically important but has been reported variably. Our aim was to define its prevalence and spectrum and to identify hematologic predictors, specifically age, hemoglobin level (Hb), platelet count (PLT), mean platelet volume (MPV), and platelet mass index (PMI).
Methods. This retrospective, single-center study evaluated all newly diagnosed leukemia patients between January 2023 and March 2025. All patients were examined by an ophthalmologist at the time of diagnosis and, if present, ocular involvement was identified.
Results. Among 78 pediatric patients, ocular involvement was present in 17 of 78 patients (21.8%). The most common ocular manifestation was retinal hemorrhage (16.7%). Ocular involvement was more frequent in acute myeloid leukemia (AML) than in acute lymphoblastic leukemia (ALL) (46.7% vs. 15.9%, p= 0.016). Older age (for ocular involvement: median 13 years [6–15] vs. 5 years [3–11], p = 0.006; for retinal hemorrhage: median 14 years [10–15] vs. 5 years [3–11], p = 0.001) and lower hemoglobin (for ocular involvement: 6.68 ± 2.31 g/dL vs. 8.46 ± 2.47 g/dL, p = 0.01; for retinal hemorrhage: 6.33 ± 2.26 g/dL vs. 8.43 ± 2.46 g/dL, p= 0.006) were associated with a higher risk. In multivariate models, age and Hb were independent predictors of hemorrhage (age: odds ratio [OR] 1.29, 95% confidence interval [CI] 1.10–1.52 per year; Hb: OR 0.60, 95% CI 0.38–0.95 per g/dL). ROC analyses showed that age provided the best discrimination (area under the curve [AUC] 0.796; 95% CI 0.651–0.940; cut-off ≥10 years: 73% sensitivity, 70% specificity), followed by Hb (AUC 0.756; 95% CI 0.604–0.908; cut-off 6.95 g/dL: sensitivity 76%, specificity 76%), whereas PLT showed weaker discrimination (AUC 0.682; 95% CI 0.553–0.812; cut-off 48,000/mm³: sensitivity 62%, specificity 65%).
Conclusion. Approximately one in five children had ocular involvement at diagnosis, most commonly retinal hemorrhage. Age and hemoglobin independently predicted retinal hemorrhage and provided useful discrimination. These data support a “hemoglobin-first” triage that prioritizes initial and follow-up ocular fundus testing in older children and those with an Hb ≲7 g/dL, with external validation of the proposed thresholds warranted.
Keywords: childhood, acute leukemia, ocular involvement, retinal hemorrhage
Introduction
Leukemia is the most common malignancy in childhood and accounts for approximately one third of pediatric cancers worldwide.1,2 In recent decades, survival rates have improved significantly due to advances in risk stratification and therapy. Nevertheless, the challenge of extramedullary involvement, particularly ocular manifestations, remains a critical clinical problem.3,4
Ocular involvement in pediatric leukemias has a complex spectrum and can occur at diagnosis, during therapy, or at relapse. These manifestations can be seen either directly (primary) or secondarily. Primary involvement involves direct infiltration of leukemic cells into ocular tissues, leading to findings such as proptosis, leukemic retinopathy, and optic neuropathy. Secondary effects occur due to hematologic abnormalities such as anemia and thrombocytopenia, resulting in retinal hemorrhages and papilledema.5,6 Although direct leukemic infiltration of ocular structures is relatively rare, it has a significant impact on visual function and may even be the first sign of leukemia. Conversely, secondary ocular complications such as retinal hemorrhages and papilledema are among the most frequently reported findings. These are often the result of profound cytopenias or hyperviscosity, particularly in acute myeloid leukemia (AML) and advanced disease.4 A significant proportion of ocular manifestations are asymptomatic and can only be identified by systematic ophthalmologic examination. This emphasizes the importance of routine ophthalmologic examinations in all newly diagnosed patients.
The prevalence of ocular involvement at diagnosis of pediatric leukemia, as reported in the literature, varies widely, ranging from 10% to 35%.4,7-9 These findings are more common in older children, in patients with AML, and in patients with severe anemia or marked thrombocytopenia. Most studies do not show a direct impact of ocular involvement at diagnosis on overall survival.10,11 However, the presence of such findings may indicate a more advanced stage of disease and therefore warrants careful clinical monitoring.7 With these considerations in mind, regular ophthalmologic examination at the time of diagnosis is increasingly recommended to detect and monitor ocular complications early, particularly in high-risk subgroups. Early detection and intervention are crucial for preventing irreversible visual impairment and enhancing the quality of life for pediatric leukemia survivors.
In this retrospective, single-center study, we aimed to evaluate the prevalence and spectrum of ocular involvement at the time of diagnosis in children with acute leukemia and to analyze its association with clinical and hematological parameters.
Materials and Methods
Study design and patient population
This retrospective, single-center study was conducted at Ankara Etlik City Hospital in Ankara, Türkiye. The medical records of children diagnosed with leukemia were reviewed between January 2023 and March 2025. A total of 78 patients aged 0–18 years were included in the analysis.
Inclusion and exclusion criteria
We included pediatric patients aged 0–18 years diagnosed with acute lymphoblastic leukemia (ALL) and AML at our center between 2023 and 2025. Eligible patients underwent a complete ophthalmologic examination at the time of diagnosis. The diagnosis of leukemia relied on hematologic, morphologic, and immunophenotypic criteria. Only patients with complete medical and laboratory records were included.
Patients were excluded if the diagnosis was made outside our center without an ophthalmologic examination being performed at the time of diagnosis, if they had concomitant ocular or systemic diseases that could influence the ophthalmologic findings (e.g. congenital ocular anomalies, diabetes mellitus, hypertension, sickle cell anemia, or coagulopathies), if they had suffered ocular trauma or intraocular surgery in the past, or if they had infectious diseases known to cause ocular involvement (e.g. toxoplasmosis, cytomegalovirus retinitis). In addition, patients diagnosed with mixed phenotype acute leukemia, chronic myeloid leukemia, or relapse cases were not included in the study.
Data collection
Demographic variables (age at diagnosis and sex), leukemia subtype, and the risk group defined in the protocol were recorded. Baseline complete blood counts including hemoglobin (Hb), platelet count (PLT), white blood cell (WBC) count, and mean platelet volume (MPV) were obtained at diagnosis prior to any transfusion and therapy.
Platelet Mass Index (PMI): As a bleeding-related composite parameter, platelet mass index was calculated as PMI = (MPV × PLT) / 1000, where MPV is reported in femtoliters (fL) and PLT in ×10⁹/L. The PMI was calculated using the same baseline complete blood count obtained at diagnosis and analyzed in the regression models as a continuous candidate predictor of bleeding.
Ophthalmological examination
At the time of leukemia diagnosis, all patients underwent a comprehensive ophthalmological evaluation performed by an experienced ophthalmologist. The assessment included best-corrected visual acuity measurement (performed with age-appropriate methods when feasible), ocular motility testing, anterior segment examination using slit-lamp biomicroscopy, and dilated fundus examination via indirect ophthalmoscopy after pharmacological mydriasis.
Ocular involvement was documented systematically for each eye and classified as follows:
- Retinal hemorrhage: intraretinal, preretinal, or subhyaloid hemorrhages observed in the posterior segment
- Retinal leukemic infiltration: yellow-white, ill-defined retinal lesions suggestive of leukemic cell accumulation
- Swollen optic disc: optic disc elevation consistent with papilledema or optic disc edema
- Retinal detachment: separation of the neurosensory retina from the underlying retinal pigment epithelium
- Cotton wool spots: localized retinal nerve fiber layer infarcts appearing as fluffy white patches
- Optic disc pallor: pale appearance of the optic nerve head, indicative of optic atrophy or ischemia
- Macular pallor: diminished coloration of the macula, potentially reflecting ischemia or degeneration
- Subconjunctival hemorrhage: well-demarcated hemorrhage beneath the conjunctiva, visible on anterior segment examination
All findings were recorded during the initial ophthalmic assessment. Patients without any ocular involvement were also documented accordingly. Fundus photography or optical coherence tomography (OCT) was performed when clinically indicated to support the diagnostic evaluation.
Definition of Ocular Involvement: Ocular involvement was defined as the presence of any abnormal ophthalmologic finding identified during a comprehensive eye examination at the time of leukemia diagnosis and considered attributable to leukemia or leukemia-related hematologic abnormalities. This definition encompassed both primary ocular involvement, reflecting direct leukemic infiltration of ocular tissues (e.g., retinal leukemic infiltration and optic disc infiltration), and secondary ocular involvement, resulting from systemic hematologic disturbances such as anemia, thrombocytopenia, or hyperviscosity (e.g., retinal hemorrhage, papilledema, and cotton wool spots). Patients without any of these findings were classified as having no ocular involvement.
Statistical analysis
Statistical analyses were performed using SPSS version 22.0 (IBM Corp., Armonk, NY). Patients were grouped into subgroups according to the presence of ocular involvement and hemorrhage. Continuous variables were tested for normality and presented as mean ± standard deviation when normally distributed, and as median (Q1–Q3) when non-normally distributed. Comparisons between groups were performed using the t-test for independent samples or the Mann-Whitney U-test for continuous variables and the chi-square test or Fisher’s exact test for categorical variables.
Univariate and multivariate logistic regression analyses were performed to identify independent predictors of ocular involvement and hemorrhage. Odds ratios (OR) with 95% confidence intervals (CI) were reported. Model calibration was assessed using the Hosmer–Lemeshow goodness-of-fit test, model discrimination was evaluated based on the percentage of correctly classified cases from the classification table, and model explanatory performance was quantified using Nagelkerke R². Variables with p < 0.20 in the univariate analysis were considered candidate variables and were included in the multivariate logistic regression model. Multicollinearity among candidate variables was assessed using the variance inflation factor (VIF) derived from collinearity diagnostics in a linear regression model including all candidate predictors. Variables showing substantial multicollinearity were identified and evaluated before inclusion in the multivariate logistic regression model. Because PMI is derived from platelet count and mean platelet volume, it showed severe multicollinearity and was therefore excluded from the final multivariate model. The discriminatory ability of hemoglobin, platelet count, and age for predicting hemorrhage was evaluated using receiver operating characteristic (ROC) curve analysis. The area under the curve (AUC), sensitivity, specificity, and optimal cut-off values were calculated, and optimal cut-off points were determined using the Youden index.
Ethical approval
This study was approved by the local institutional ethics committee (AEŞH-BADEK1-2025-535) and conducted in accordance with the principles of the Declaration of Helsinki.
Results
At the time of diagnosis, a total of 78 pediatric patients (45 boys and 33 girls; median age 6 years [3-13]) with acute leukemia were evaluated. Of these patients, 63 (80.8%) were diagnosed with ALL and 15 (19.2%) with AML. The baseline demographic and laboratory data of the study population are summarized in Table I.
|
Percentages for ALL and AML cases are calculated out of the total study population. Percentages for B-cell ALL and T-cell ALL are calculated within the ALL group. Percentages for risk groups are calculated within their respective leukemia subtypes (B-cell ALL, T-cell ALL, or AML). ALL: acute lymphoblastic leukemia; AML: acute myeloid leukemia. |
|
| Table I. Demographic and clinical characteristics of the study population. | |
| Variable |
|
| Age (years), median (Q1-Q3) |
|
| Sex, n (%) | |
| Male |
|
| Female |
|
| Leukemia subtype, n (%) | |
| Acute lymphoblastic leukemia |
|
| B-cell ALL |
|
| Standard risk |
|
| Medium risk |
|
| High risk |
|
| T-cell ALL |
|
| Medium risk |
|
| High risk |
|
| Acute myeloid leukemia |
|
| Standard risk |
|
| Medium risk |
|
| High risk |
|
In the 78 patients who participated in the study, the median WBC count was 13,375/mm³ (3,500–51,310), the mean Hb level was 8.07 g/dL (standard deviation: 2.53), the median PLT count was 58,500/mm³ (25,000–136,000), the median MPV level was 10.1 fL (9.3–10.8) and the median PMI value was 604 (243–1,210). The comparative results for the ALL and AML subgroups are shown in Table II.
| ALL: acute lymphoblastic leukemia; AML: acute myeloid leukemia; Hb: hemoglobin; MPV: mean platelet volume; PLT: platelet; PMI: platelet mass index; WBC: white blood cells. | ||||
| Table II. Baseline hematologic parameters at diagnosis by leukemia subtype (ALL vs. AML). | ||||
|
|
|
|
|
|
| WBC (/mm³) (median, Q1-Q3) |
(3,905–46,805) |
(2,525–98,495) |
(3,500–51,310) |
|
| Hb (g/dL) (mean, SD) |
|
|
|
|
| PLT (/mm³) (median, Q1-Q3) |
(24,000–131,500) |
(38,500–127,000) |
(25,000–136,000) |
|
| MPV (fL) (median, Q1-Q3) |
|
|
|
|
| PMI index (median, Q1-Q3) |
(241–1,202) |
(409.70–1,119) |
(243.60–1,210) |
|
Seventeen of the 78 patients (21.8%) with leukemia presented with ocular involvement. Of these findings, 70.5% were secondary manifestations and 29.5% represented primary leukemic infiltration. The most common ocular manifestation was retinal hemorrhage, which was observed in 13 patients (16.7%), followed by retinal infiltration in 4 patients (5.1%). Less common findings were cotton wool spots, papilledema, nasal blurring of the optic disc margin, and mild macular pallor, each observed in a single patient (1.3%) (Table III). Ocular involvement was observed in 10 of 63 patients with ALL (15.9%) and in 7 of 15 patients with AML (46.7%) (p=0.016). Retinal hemorrhages were observed in 6 patients with ALL (9.5%) and in 7 patients with AML (46.7%), with a significantly higher incidence in the AML group (p= 0.002). When analyzed by leukemia subtype, retinal hemorrhages were observed in 5 of 53 patients with B-cell ALL (9.4%) and in 1 of 10 patients with T-cell ALL (10%), with no statistically significant difference between the groups. Furthermore, no significant difference in ocular involvement was found when comparing the risk groups for ALL and AML. On the other hand, the time from symptom onset to hospitalization did not differ between patients with and without ocular involvement (median 13 days [3–60] vs. median 15 days [3–90], respectively; p = 0.300).
| Percentages are calculated based on the total number of patients (n=78). Since many patients had no ocular involvement, the sum of the percentages is less than 100%. | |
| Table III. Distribution of ocular involvement detected at the time of leukemia diagnosis (N=78). | |
| Findings |
|
| Retinal hemorrhage |
|
| Retinal leukemic infiltration |
|
| Nasal blurring of the optic disc |
|
| Retinal detachment |
|
| Cotton wool spot |
|
| Optic disc pallor |
|
| Macular pallor |
|
| Subconjunctival hemorrhage |
|
Patients with any ocular involvement were significantly older than those without ocular involvement (median age 13 years [6–15] vs. 5 years [3–11.5], p=0.006). Similarly, when retinal hemorrhage was evaluated as a specific ocular manifestation, patients with hemorrhage had a higher median age compared with those without hemorrhage (median age 14 years [10–15] vs. 5 years [3–11], p = 0.001).
In the comparison between patients with and without retinal hemorrhage, the Hb level (6.33 ± 2.26 g/dL vs. 8.43 ± 2.46 g/dL, p = 0.006) and platelet counts (median 42,000/mm³ [22,000–55,000] vs. 68,000/mm³ [26,000–157,000], p = 0.039) were significantly lower in the hemorrhage group. In contrast, MPV values were higher in patients with hemorrhage (median 11.0 fL [10.3–11.2] vs. 10.0 fL [9.2–10.5], p = 0.008) (Table IV). In multivariate logistic regression analysis including age, hemoglobin, platelet count and MPV; only older age and lower Hb levels remained independently associated with retinal hemorrhage (age: OR 1.29, 95% CI 1.10–1.52, p=0.002; Hb: OR 0.60, 95% CI 0.38–0.95, p=0.030). The logistic regression model was statistically significant (χ² = 25.840, p < 0.001), showed acceptable calibration according to the Hosmer–Lemeshow goodness-of-fit test (p = 0.387), and correctly classified 93.6% of the cases (Nagelkerke R² = 0.475) (Table V). Similarly, in patients with ocular involvement, Hb levels (6.68 ± 2.31 g/dL vs. 8.46 ± 2.47 g/dL, p = 0.01) and platelet counts (median 42,000/mm³ [22,000–75,000] vs. 68,000/mm³ [28,000–157,000], p = 0.050) were significantly lower compared to those without ocular involvement, whereas MPV values (median 10.4 fL [10.0–11.2] vs. 10.0 fL [9.2–10.5], p = 0.028) were higher (Table IV). In multivariate logistic regression analysis including age, hemoglobin, platelet count and MPV, older age and lower Hb levels were independently associated with ocular involvement (age: OR 1.19; 95% CI, 1.05–1.36; p=0.007; Hb: OR 0.69; 95% CI, 0.49–0.98; p=0.037). The logistic regression model was statistically significant (χ² = 18.797, p = 0.001), showed acceptable calibration according to the Hosmer–Lemeshow goodness-of-fit test (p = 0.488), and correctly classified 85.9% of cases (Nagelkerke R² = 0.330) (Table V).
| Hb: hemoglobin; MPV: mean platelet volume; PLT: platelet; PMI: platelet mass index; WBC: white blood cells. | ||||||
| Table IV. Baseline hematologic parameters at diagnosis by retinal hemorrhage status and ocular involvement. | ||||||
|
|
|
|
|
|
|
|
| WBC (/mm³) (median, Q1–Q3) |
(3,860–46,750) |
(2,790–130,000) |
|
(3,950–46,750) |
(2,790–130,000) |
|
| Hb (g/dL) (mean, SD) |
|
|
|
|
|
|
| PLT (/mm³) (median, Q1–Q3 ) |
(26,000–157,000) |
(22,000–55,000) |
|
(28,000–157,000) |
(22,000–75,000) |
|
| MPV (fL) (median, Q1–Q3) |
(9.20-10.50) |
(10.30-11.20) |
|
(9.20-10.50) |
(10.00-11.20) |
|
| PMI (median, Q1–Q3 ) |
(249.60–1,460) |
(240.00–603.00) |
|
(252.50–1,460) |
(240.00–765.00) |
|
|
Variables not significant in univariate analysis (WBC and MPV×PLT) were not included in the multivariate model. CI: confidence interval; Hb: hemoglobin; MPV: mean platelet volume; OR: odds ratio; PLT: platelet; PMI: platelet mass index; WBC: white blood cells. |
||||
| Table V. Logistic regression analysis of parameters associated with retinal hemorrhage and ocular involvement. | ||||
| Variable |
|
|
|
|
| Age (years) |
|
|
|
|
| Hb (g/dL) |
|
|
|
|
| PLT (x103/µL) |
|
|
|
p=0.507 |
| MPV (fL) |
|
|
|
p=0.786 |
| WBC (x103/µL) |
|
|
|
|
| PMI |
|
|
||
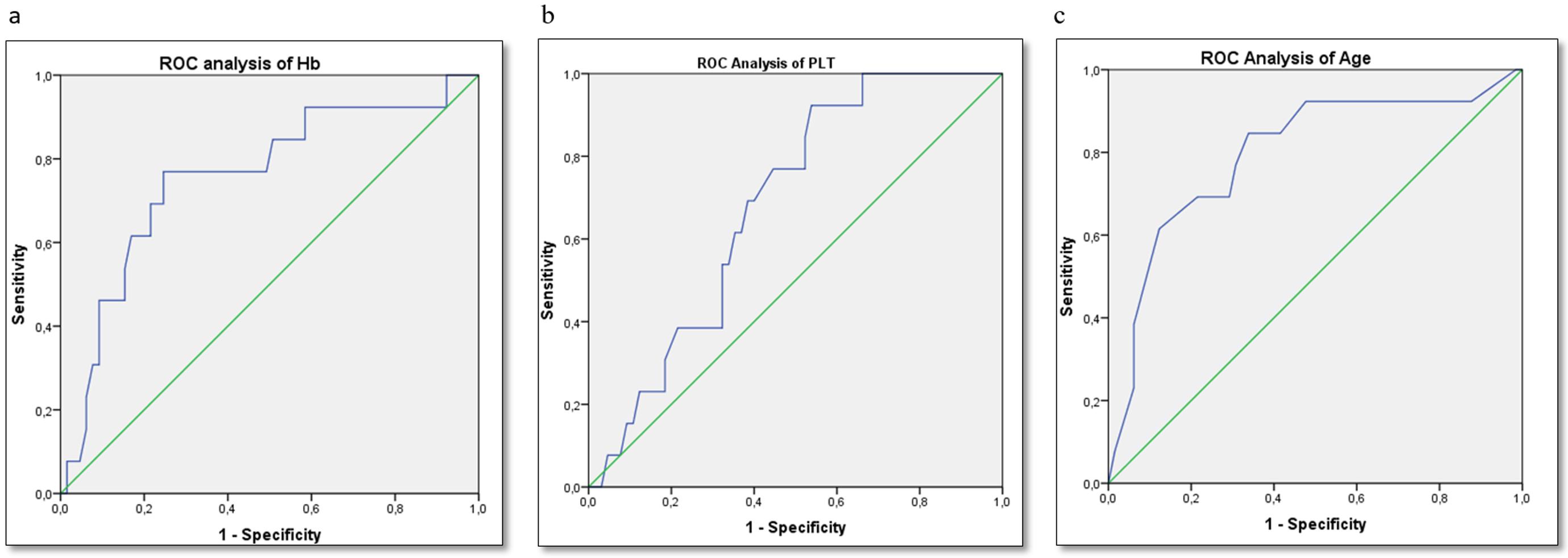
ROC curve analysis revealed that age was a significant predictor of retinal hemorrhage (AUC=0.796; 95% CI, 0.651–0.940; p=0.001), with a cut-off point of 10 years resulting in a sensitivity of 73% and a specificity of 70%. Hemoglobin also showed good discrimination (AUC=0.756, 95% CI: 0.604–0.908, p=0.004), with a cut-off value of 6.95 g/dL yielding a sensitivity of 76% and a specificity of 76%. The platelet count showed a moderate discriminative performance (AUC=0.682, 95% CI: 0.553–0.812, p=0.039), and a cut-off of 48,000/mm³ provided a sensitivity of 62% and a specificity of 65%. The ROC analysis showed that age was the strongest discriminator of retinal hemorrhage (AUC=0.796; 95% CI, 0.651–0.940; p=0.001), compared with Hb (AUC=0.756; 95% CI, 0.604–0.908; p=0.004) and platelet count (AUC=0.682; 95% CI, 0.553–0.812; p=0.039) (Fig. 1). These results support the conclusion that age and Hb values together represent an independent risk factor for the prediction of retinal hemorrhage, while PLT may serve as a complementary parameter with potential clinical utility.
Discussion
The prevalence of ocular manifestations in pediatric patients diagnosed with acute leukemia is of great concern, as several studies emphasize the need for a thorough ophthalmologic examination at diagnosis. In this study, 78 pediatric acute leukemia patients were evaluated, 21.8% of whom had abnormal ocular involvement at diagnosis. These findings are consistent with the existing literature, which reports a prevalence of ocular involvement ranging from 10 to 35% in acute leukemia cases.4,5,7,9 Furthermore, a recent meta-analysis including 2,989 patients from 14 studies, found a prevalence of 20.32% for ocular involvement in newly diagnosed leukemia, underscoring the importance of ocular examinations in this patient group.4
The most frequently observed ocular manifestation in this cohort was retinal hemorrhage, which was noted in 13 patients (16.7%). This is consistent with the findings of Bitirgen et al. who described retinal hemorrhages as round or flame-shaped lesions that may show the accumulation of leukemic cells or platelet-fibrin aggregates.9 They pointed out that such hemorrhagic events usually resolve with remission, emphasizing the dynamic relationship between underlying disease status and ocular health. Understanding these presenting ocular signs is critical as they may provide important prognostic insights into the behavior of the hemorrhagic disease and potential clinical outcomes.8,12
Age showed the best discrimination for hemorrhage (AUC = 0.796; 95% CI, 0.651–0.940) and remained independently associated after adjustment, with a prespecified threshold of ≥10 years yielding a sensitivity of 73% and specificity of 70%. This is consistent with pediatric reports showing that ocular involvement increases with age at diagnosis- particularly in AML- even when hematologic indices are comparable.10 As age cut-offs in pediatrics are not standardized, our threshold of ≥10 years should be considered provisional and subject to external validation.7
Hemoglobin demonstrated moderate discrimination (AUC = 0.756; 95% CI, 0.604–0.908) with an optimal cut-off value of 6.95 g/dL (76% sensitivity/specificity), which closely follows current restrictive transfusion guidelines for stable hospitalized patients.13 Pediatric acute leukemia series also demonstrates an association between lower Hb levels and retinal hemorrhages. For example, Benvenuto et al. reported mean Hb level of 7.4 g/dL in children with retinal hemorrhages at diagnosis, confirming the validity of our cut-off value.7 Given the heterogeneity of the cohorts (e.g. suggestions of ≤9.9 g/dL with weaker AUC), external validation of the 7 g/dL threshold is warranted.14 In practice, children with an Hb level <7 g/dL - especially those who are older or symptomatic - should be prioritized for initial and follow-up ocular fundus examinations, while transfusion decisions remain individualized and guideline-driven.13
Several studies have identified hematologic laboratory parameters as key correlates of retinal hemorrhages, with anemia and, to a lesser extent, thrombocytopenia as notable examples.15-17 Of these factors, Hb level remains the most reliable independent risk factor. This study confirms that lower hemoglobin levels are independently associated with the presence of retinal hemorrhage at the time of leukemia diagnosis. Similar associations between severe anemia and hemorrhagic retinal manifestations have been consistently reported in pediatric acute leukemia cohorts.7,11 Furthermore, comparisons between pediatric and mixed-age cohorts indicate an age-related gradient in ocular manifestations, which supports the plausibility of age-dependent susceptibility. Nevertheless, pediatric-specific age thresholds are not standardized. Hence, our threshold of 10 years or older should be considered hypothesis-generating and requires external validation. Finally, platelet indices showed weak and non-independent performance in our models. This reflects studies in which platelets provide limited discrimination once hemoglobin, age, or disease subtype are taken into account.7
Severe anemia reduces retinal oxygenation, promoting hypoxia-induced capillary fragility and disruption of the inner blood-retinal barrier; this biologically explains the stronger association between low Hb and hemorrhage. The rheology of leukemic blood (e.g. leukostasis / viscosity) may further impair microvascular flow, while platelet-fibrin microthrombi (Roth spots) mark endothelial damage. In AML, choroidal/leukemic infiltration may also impair choriocapillaris flow, triggering retinal pigment epithelial pump failure and hemorrhagic/exudative phenotypes.11 Taken together, these mechanisms support a “hemoglobin-first” triage for ophthalmologic monitoring and explain why platelet indices offer little additional discriminatory power once Hb (and age) are taken into account.
In our cohort, MPV differed between groups in univariate analysis but was not independent after adjustment. In contrast, age and hemoglobin remained independent predictors, while platelet count, like MPV, was not an independent risk factor. Furthermore, neither the platelet mass index nor the WBC count showed any association with hemorrhage. This observed pattern is consistent with findings in pediatric leukemia suggesting that anemia is the most important hematologic determinant of ocular/retinal hemorrhage, while platelet-based metrics (PLT, MPV, and thus PMI) provide limited additional value when Hb and age are taken into account.7,10,14,18 Taken together, these results support a “hemoglobin-first” triage approach for ocular involvement in pediatric acute leukemia. On the other hand PLT/MPV parameters serve as complementary indicators. Nevertheless, given biological plausibility and potential timing/assay variability, MPV and PMI should be reassessed in adequately powered, prospective, leukemia-specific cohorts with standardized CBC timing and ophthalmic endpoints.
At presentation, abnormal ocular involvement was more frequent and/or pronounced in AML than in ALL. No significant differences were observed between the various immunophenotypic subtypes of ALL (B-ALL vs. T-ALL). Clinically, this pattern supports prioritizing baseline and repeated fundoscopic examinations during diagnosis and induction in AML, particularly in older or markedly anemic patients. Prompt supportive care—correcting anemia and managing coagulopathy—should also be provided to reduce ocular complications. In acute leukemia, a universal screening approach remains appropriate regardless of immunophenotype. Ophthalmic surveillance should mainly be stratified by hematologic burden (especially hemoglobin level) and age, rather than by B-ALL or T-ALL classification.
Our study has several limitations; including its retrospective nature and the retrospective collection of data. Additionally, it is a single-center study with a relatively small patient cohort. Although patients underwent ophthalmologic examinations within 24-48 hours of diagnosis, these examinations were performed by different ophthalmologists. Additionally, we were unable to perform a survival analysis comparing patients with and without ocular involvement.
Conclusion
Abnormal ocular manifestations occur in about a quarter of children with newly diagnosed acute leukemia, with retinal hemorrhages and leukemic infiltrations being the most common findings. Ocular involvement is particularly increased in AML, in older children, and in children with lower hemoglobin levels. We recommend routine ophthalmologic examinations at the diagnosis of acute leukemia, even if the patient is asymptomatic. A multidisciplinary management approach, incorporating both pediatric hematology and ophthalmology, is crucial for timely intervention and to optimize patient outcomes in this vulnerable population. This study may guide the re-evalution of transfusion policies in acute leukemia with ocular involvement, particularly in retinal hemorrhage, in the future.
Acknowledgements
This study was conducted solely at Ankara Etlik City Hospital (Department of Pediatric Hematology–Oncology). We thank our patients and their families, and the ward and ophthalmology staff for routine clinical care. No additional individuals or institutions contributed beyond standard clinical duties.
Ethical approval
The study was approved by Ankara Etlik City Hospital Ethics Committee (date: 03.09.2025, number: AEŞH-BADEK1-2025-535).
Source of funding
The authors declare the study received no funding.
Conflict of interest
The authors declare that there is no conflict of interest.
References
- Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021; 71: 209-249. https://doi.org/10.3322/caac.21660
- Liu W, Fang J, Zhu M, Zhou J, Yuan C. Global, regional, and national burden of childhood leukemia from 1990 to 2021. BMC Pediatr 2025; 25: 571. https://doi.org/10.1186/s12887-025-05847-7
- Kim H, Yoon SH, Kang S, et al. Improved survival in pediatric acute lymphoblastic leukemia through therapy intensification based on minimal residual disease and protocol-driven early response risk classification. Blood Res 2025; 60: 40. https://doi.org/10.1007/s44313-025-00085-3
- Nazzicone K, Kim R, Fine A, Pucchio A, Wheaton L, Law C. Ocular involvement in newly diagnosed pediatric leukemia: A systematic review and meta-analysis. Pediatr Investig 2025; 9: 150-159. https://doi.org/10.1002/ped4.12473
- Sayadi J, Gouider D, Allouche Y, et al. Ophthalmic manifestations of newly diagnosed acute leukemia patients in a Tunisian cohort. Clin Ophthalmol 2022; 16: 3425-3435. https://doi.org/10.2147/OPTH.S365648
- Russo V, Scott IU, Querques G, Stella A, Barone A, Delle Noci N. Orbital and ocular manifestations of acute childhood leukemia: clinical and statistical analysis of 180 patients. Eur J Ophthalmol 2008; 18: 619-623. https://doi.org/10.1177/112067210801800420
- Benvenuto F, Sgroi M, Guillen SS, Ancona D, Fandiño A. Ocular findings in children with acute leukemia at a tertiary care center in South America. Oman J Ophthalmol 2022; 15: 159-162. https://doi.org/10.4103/ojo.ojo_347_20
- Mirshahi R, Ghassemi F, Koochakzadeh L, et al. Ocular manifestations of newly diagnosed acute leukemia patients. J Curr Ophthalmol 2022; 34: 100-105. https://doi.org/10.4103/joco.joco_10_21
- Bitirgen G, Belviranli S, Caliskan U, Tokgoz H, Ozkagnici A, Zengin N. Ophthalmic manifestations in recently diagnosed childhood leukemia. Eur J Ophthalmol 2016; 26: 88-91. https://doi.org/10.5301/ejo.5000647
- Orhan B, Malbora B, Akça Bayar S, Avcı Z, Alioğlu B, Özbek N. Ophthalmologic findings in children with leukemia: a single-center study. Turk J Ophthalmol 2016; 46: 62-67. https://doi.org/10.4274/tjo.03880
- Laimon DN, Sakr DH, Atef B, Shaaban Y. Highlights of ophthalmological manifestations in newly diagnosed acute leukemia: a correlation with hematological parameters. Ann Hematol 2024; 103: 3519-3533. https://doi.org/10.1007/s00277-024-05861-2
- Ohkoshi K, Tsiaras WG. Prognostic importance of ophthalmic manifestations in childhood leukaemia. Br J Ophthalmol 1992; 76: 651-655. https://doi.org/10.1136/bjo.76.11.651
- Carson JL, Stanworth SJ, Guyatt G, et al. Red blood cell transfusion: 2023 AABB international guidelines. JAMA 2023; 330: 1892-1902. https://doi.org/10.1001/jama.2023.12914
- Chegondi M, Vijayakumar N, Billa RD, Badheka A, Karam O. Performance of platelet mass index as a marker of severity for sepsis and septic shock in children. J Pediatr Intensive Care 2021; 12: 228-234. https://doi.org/10.1055/s-0041-1731434
- Liu TYA, Johnson TV, Barnett BP, Scott AW. Evolution of leukemic retinal hemorrhages documented by spectral-domain OCT and color fundus photography. Ophthalmol Retina 2018; 2: 494-501. https://doi.org/10.1016/j.oret.2017.08.014
- abu el-Asrar AM, al-Momen AK, Kangave D, Harakati MS, Ajarim DS. Correlation of fundus lesions and hematologic findings in leukemic retinopathy. Eur J Ophthalmol 1996; 6: 167-172. https://doi.org/10.1177/112067219600600213
- Soman S, Kasturi N, Srinivasan R, Vinod KV. Ocular manifestations in leukemias and their correlation with hematologic parameters at a tertiary care setting in South India. Ophthalmol Retina 2018; 2: 17-23. https://doi.org/10.1016/j.oret.2017.05.009
- Deger I, Ertuğrul S, Kaya IK, Tanrıverdi Yılmaz S, Yolbaş I. Can platelet count, platelet mass index and mean platelet volume be parameters in retinopathy of prematurity? Eastern Journal of Medicine 2022; 27: 513-518. https://doi.org/10.5505/ejm.2022.34545
Copyright and license
Copyright © 2026 The Author(s). This is an open access article distributed under the Creative Commons Attribution License (CC BY), which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is properly cited.









