
Abstract
Background. Children with a solitary functioning kidney (SFK) are at risk for hypertension and kidney injury despite compensatory renal growth. However, the relationship between compensatory enlargement and blood pressure abnormalities remains controversial. This study is an exploratory observational study aimed at assessing ambulatory blood pressure monitoring (ABPM) parameters in children with an SFK and to evaluate the relationship between compensatory kidney enlargement and blood pressure indices.
Methods. Thirty-three children aged 6–18 years with an SFK (22 renal agenesis, 11 atrophic kidneys) were evaluated. Compensatory enlargement was defined as kidney length >97.5th percentile for height. All participants underwent anthropometric assessment, serum creatinine measurement, estimated glomerular filtration rate (GFR) calculation, and 24-hour ABPM. ABPM values were expressed as standard deviation scores (SDS) adjusted for age and sex.
Results. Compensatory enlargement was present in 17 (51.5%) patients. Those with compensatory enlargement showed significantly higher 24-hour systolic BP SDS (0.64±1.07 vs. –0.22±1.03, p=0.024), nighttime systolic BP SDS (1.36±1.04 vs. 0.38±0.93, p=0.008), nighttime diastolic BP SDS (1.42±1.17 vs. 0.48±0.70, p=0.009), and nighttime MAP SDS (1.43±0.99 vs. 0.48±0.84, p=0.006). Kidney length SDS correlated positively with 24-h systolic BP SDS (r=0.44, p=0.01) and nighttime MAP SDS (r=0.45, p=0.009). Logistic regression analysis revealed that compensatory enlargement independently predicted elevated blood pressure (OR 10.06, 95% CI 1.03–97.77, p=0.047) after adjustment for age, height SDS, and weight SDS.
Conclusions. Compensatory hypertrophy in SFK may not be entirely benign and could reflect an adaptive process associated with altered blood pressure regulation. Higher nocturnal blood pressure in patients with compensatory enlargement may suggest subclinical hemodynamic stress. These findings suggest that children with compensatory kidney enlargement may exhibit subtle alterations in ambulatory blood pressure patterns, warranting further investigation in larger longitudinal studies.
Keywords: ambulatory blood pressure measurement, compensatory hypertrophy, hypertension, kidney length, renal adaptation, solitary functioning kidney
Introduction
Solitary functioning kidney (SFK) refers to an anatomical or functional absence of one kidney. A rough estimation of SFK has been reported as one in every 1400 births.1,2 SFK can result from a variety of congenital and acquired conditions, ranging from renal agenesis, cystic dysplasia and multicystic dysplastic kidney (MCDK) to post-nephrectomy states due to congenital kidney and urinary tract abnormalities (CAKUT) or tumors or atrophic kidneys due to renal scarring.
Despite the prevailing belief that having only one SFK was no worse than having two kidneys, mounting evidence now indicates that patients with an SFK may experience less favorable long term clinical outcomes than previously assumed and living with an SFK may expose these people to certain risks such as hypertension and kidney injury.3-9 Elevated blood pressure is an important risk factor in terms of preservation of kidney functions even in people with two kidneys. The prevalance of masked and ambulatory hypertension in SFK has been reported as approximately 15% and 27%, respectively in different studies.10 The assessment of blood pressure in children is commonly based on casual blood pressure measurement, whereas in recent years ambulatory blood pressure monitoring (ABPM) has been widely used in the assessment of high blood pressure in children. Although there are opinions against the routine use of ABPM in patients with SFK10, there has been an increasing number of reports encouraging the use of ABPM in the blood pressure monitoring of patients with SFK and these studies commonly indicate that blood pressure abnormalities may actually be more frequent than previously thought in patients with SFK.3-5,8,9,11 Limited data exists on the correlation between blood pressure and kidney size in SFK.5,12
The relationship between compensatory renal enlargement and hypertension remains unclear. While some studies suggest an inverse association between compensatory enlargement and hypertension, others report no significant relationship.3,11 In contrast, some authors have proposed that greater enlargement of the remaining kidney may be associated with higher blood pressure.5 The debate in the literatüre regarding the relationship between compensatory enlargement in SFK and blood pressure abnormality prompted us to design the current study.
In this study, we aimed to evaluate ambulatory blood pressure (ABP) profiles in children with an SFK and to investigate the relationship between compensatory kidney enlargement and ABP indices.
Material and Methods
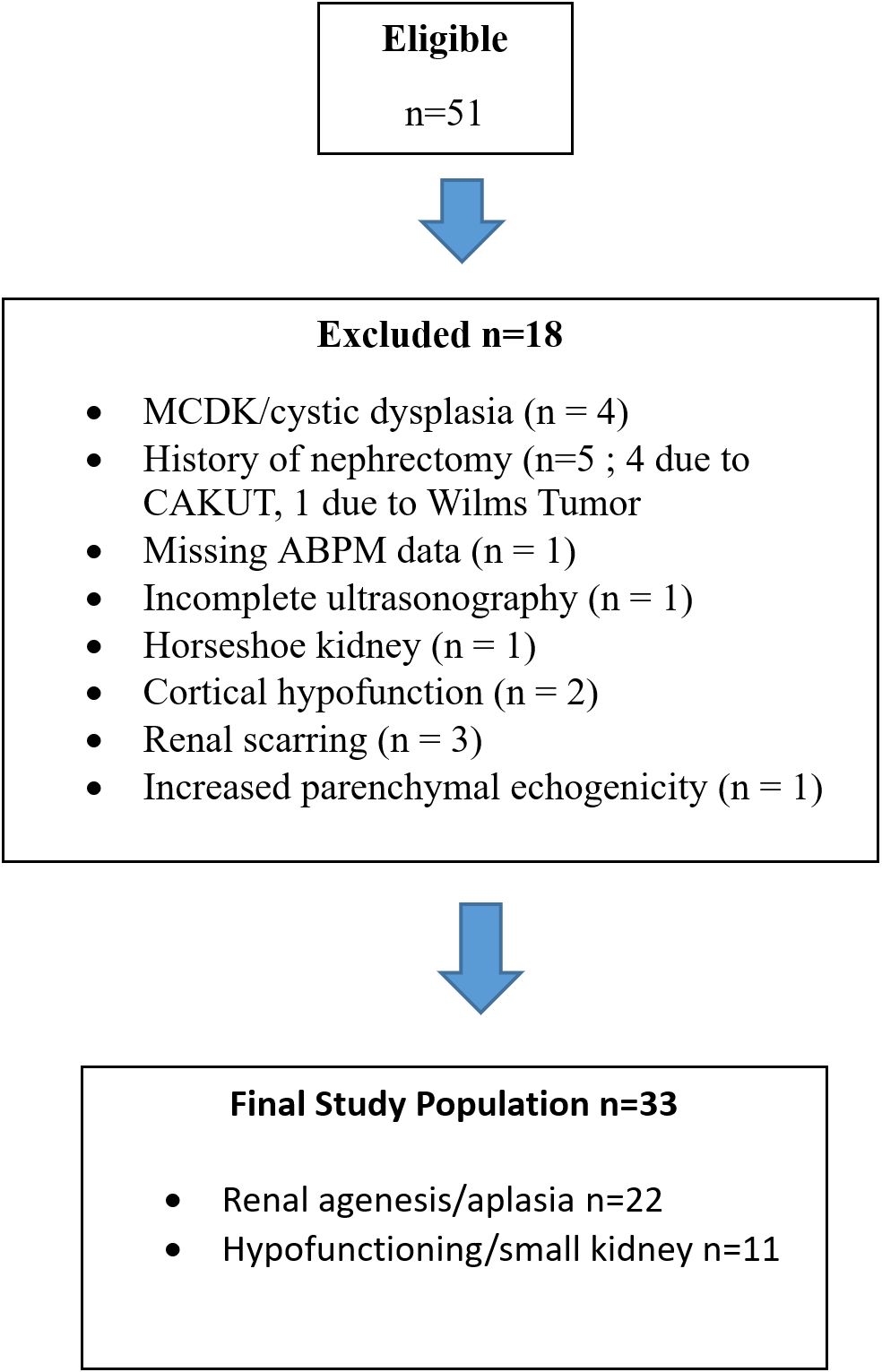
The study was conducted on children admitted to the pediatric nephrology clinic at a tertiary medical centre between January 2018 and January 2021, all were diagnosed with an SFK. All procedures contributing to this work complied with the ethical standards of the relevant national guidelines on human medical regulations and the Helsinki Declaration of 1975, as revised in 2008 and ethical approval was obtained from the hospital’s local ethics committee. Patients with an SFK between 6-18 years of age, who had not receieved antihypertensive treatment before were included as the study group. A total of 51 pediatric patients with an SFK were initially enrolled in the study. Patients who exhibited renal scarring, cysts, kidney masses or additional CAKUT in SFK were excluded. According to the study protocol, 18 patients were excluded due to conditions that could compromise the assessment: 4 with MCDK/cystic dyslasia without involution, 5 with a history of nephrectomy (4 nehprectomy due to CAKUT, 1 nehprectomy due to Wilms tumor), 1 lacking 24-hour ABPM data, 1 with incomplete ultrasonographic measurements, 1 with a horseshoe kidney, 2 with cortical hypofunction, 3 with renal scarring, and 1 with marked increased parenchymal echogenicity. Consequently, 33 patients were included in the final analysis (Fig. 1). The SFK cases included 22 patients with congenital renal agenesis/aplasia and 11 small atrophic/ hypofunctioning kidney with tracer uptake below 5 % on dimercapto succinic acid (DMSA)/ mercapto acetyl triglycine (MAG3).
In this study, the diagnosis of SFK was confirmed using renal ultrasonography and Tc-99m DMSA or Tc-99m MAG3 scintagraphy. SFK was characterized by the absence of functional kidney tissue on ultrasound and/or on DMSA/MAG3 scintigraphy (kidney with tracer uptake below 5 % on DMSA/MAG3).8 Weight (kg), height (cm), and body mass index (BMI) (kg/m2) values, along with their corresponding standard deviation scores (SDS), were collected and analyzed based on predefined norms for Turkish children.13 Serum creatinine levels were assessed and the bedside Schwartz glomerular filtration rate (GFR) equation was employed to estimate the glomerular filtration rate (eGFR).14,15 The office blood pressure measurements were conducted by a pediatric nephrologist using auscultation. Prior to measurement, the patients were given a 30-minute rest. The readings were taken at least three times on the non-dominant arm, using an appropriately sized cuff.16 For ABPM, an oscillometric device (Suntech, Morrisville, USA) was used.17 The monitoring frequency during the day was every 20 minutes, and during the night, it was every 30 minutes. To differentiate between awake and sleep periods, the patients’ self-reported sleep-wake times were recorded in a diary. Nocturnal dipping was defined as a 10% decline in mean systolic and diastolic ABP levels from day to night.18 Blood pressure load was calculated as the percentage of valid measurements above the 95th percentile of blood pressure for age, gender, and height.19 Blood pressure (BP) load parameters were analyzed as exploratory indicators of BP burden rather than as diagnostic criteria, in accordance with recent American Heart Association (AHA) recommendations. To assess BP values accurately, SD (standard deviation) scores (95th percentile correspondes to 1.645 SD) of mean systolic blood pressure (SBP), diastolic blood pressure (DBP), and mean arterial blood pressure (MAP) were calculated based on normative data presented by Wühl et al. with the “Child Metrics” computer program to standardize measurements according to age and gender (https://www.ceddcozum.com).19 Blood pressure was then categorized using the scheme suggested by Flynn et al.20
Ultrasonography
Ultrasonography was performed using a LOGIQ P9 (GE Healthcare) machine equipped with a multi-frequency 4–6 MHz probe by an experienced pediatric radiologist who was blinded to the ABPM results. Kidney measurements were obtained with the children in the supine position. Kidney length (maximum bipolar length) was measured in the coronal plane. In pediatric populations, kidney size correlates more closely with height than chronological age; therefore, kidney length SDS were calculated based on height-adjusted normative data, rather than age-based references. This approach accounts for individual variations in somatic growth and avoids misclassification in children with growth retardation or accelerated growth so compensatory enlargement of the SFK in our study was defined as a kidney length greater than the 97.5th percentile or a corresponding SDS score ≥ 1.96, based on normative data presented by Obrycki et al.21,22
Standardization of measurements according to patient height was performed using the calculator available at https://www.kidneylength.com.21,22
Statistical analysis
Statistical analyses were performed using IBM SPSS Statistics 25.0 (IBM Corp., Armonk, NY, USA). The normal distribution of the variables was evaluated using histograms and probability graphs and with Kolmogorov-Smirnov and Shapiro-Wilk tests. Descriptive analysis was performed using frequency tables for categorical variables, while means and standard deviations were used to describe normally distributed variables. Medians and quartiles (Q1–Q3) were used to describe variables with non-normal distribution. Results were evaluated with a confidence interval of 95%, and p<0.05 was considered statistically significant. Student’s t test and Mann-Whitney U test was used to compare the means and medians of continuous variables. Spearman’s Correlation Analysis was used to determine the relationship between SDS scores of ABPM parameters and kidney length SDS. The relationship between normal and elevated blood pressure with age, weight, height and presence of compensatory enlargement of SFK evaluated by univariate and multiple binary logistic regression analysis.
Results
The study included a total of 33 patients, 22 (66.7%) of whom were diagnosed with renal agenesis and 11 (33.3 %) with a small hypofunctioning kidney. Compensatory enlargement was present in 17 (51.5%) patients, whereas 16 (48.5%) patients did not demonstrate compensatory enlargement. There were no significant differences in age or anthropometric measurements and corresponding SDSs between patients with compensatory enlargement and those without. The median GFR values were similar in both groups. A significant association was observed between sex and compensatory kidney enlargement based on height-adjusted SDS values. Among female patients, 84.6% demonstrated compensatory enlargement, whereas only 30.0% of male patients showed this finding. The difference between sexes was statistically significant (χ2 = 9.41, df = 1, p = 0.002; Fisher’s exact test p = 0.004) (Table I). Among the study population, hypertension was more prevalent in patients with compensatory kidney enlargement compared to those without (47.1% vs. 12.5%). However, this difference did not reach statistical significance (Fisher’s exact test, two-sided p = 0.054).
|
SFK: Solitary functioning kidney SD: standard deviation score BMI: body mass index eGFR: estimated glomeruler filtration rate Values are presented as mean ± SD or median (Q1–Q3). Mann–Whitney U test was used for non-normally distributed variables. |
||||
| Table I. Demographic features of the patients. | ||||
|
|
|
|
||
| Sex, n (%) | Female |
|
|
|
| Male |
|
|
||
| SFK etiology, n (%) | Renal agenesis |
|
|
|
| Small non-functioning kidney |
|
|
||
| Age (years) |
|
|
|
|
| Weight (kg) |
|
|
|
|
| Weight SDS |
|
|
|
|
| Height (cm) |
|
|
|
|
| Height SDS |
|
|
|
|
| BMI (kg/m2) |
|
|
|
|
| BMI SDS |
|
|
|
|
| Creatinine (mg/dl) |
|
|
|
|
| eGFR (mL/min/1.73m2) |
|
|
|
|
Based on the results of ABPM, the group with compensatory enlargement had significantly higher 24-h systolic BP SDS (0.64±1.07 vs.-0.22±1.03 p=0.024), night systolic BP SDS (1.36±1.04 vs. 0.38±0.93 p= 0.008), night diastolic BP SDS (1.42±1.17 vs. 0.48±0.70 p= 0.009), night MAP SDS (1.43±0.99 vs. 0.48±0.84 p = 0.006) compared to the group without compensatory enlargement, respectively (Table II).
|
ABPM: ambulatory blood pressure monitör, SFK: solitary functioning kidney MAP: mean arterial pressure BP: blood pressure SD: standard deviation SDS: standard deviation scores *Mann-Whitney U Test ** Pearson Chi –square #Fisher’s Exact Test (2-tailed) Values are presented as mean ± SD or median (Q1–Q3) according to data distribution. |
||||
| Table II. Comparision of ABPM profiles according to existence of compensatory enlargement in SFK. | ||||
| BP parameters |
(n= 16) |
(n=17) |
|
|
| Office BP | Office systolic BP SD score |
|
|
|
| Office diastolic BP SD score |
|
|
|
|
| 24-h ABPM values | 24-h systolic BP SDS |
|
|
|
| 24-h diastolic BP SDS |
|
|
|
|
| 24-h MAP SDS |
|
|
|
|
| Day systolic BP SDS |
|
|
|
|
| Day diastolic BP SDS |
|
|
|
|
| Day MAP SDS |
|
|
|
|
| Night systolic BP SDS |
|
|
|
|
| Night diastolic BP SDS |
|
|
|
|
| Night MAP SDS |
|
|
|
|
| BP load and dipping* | 24-h systolic BP load (%) |
|
|
|
| 24-h diastolic BP load (%) |
|
|
|
|
| Day systolic BP load (%) |
|
|
|
|
| Day diastolic BP load (%) |
|
|
|
|
| Night systolic BP load (%) |
|
|
|
|
| Night diastolic BP load (%) |
|
|
|
|
| Systolic BP dipping |
|
|
|
|
| Diastolic BP dipping |
|
|
|
|
| BP dipping# | Dipper, n (%) |
|
|
|
| Non-dipper, n (%) |
|
|
||
| BP profile** | Normal, n (%) |
|
|
|
| HT, n (%) |
|
|
||
Patients with compensatory kidney enlargement exhibited significantly higher nighttime BP loads compared to those without compensatory enlargement. Median nighttime systolic BP load was 31% (12–70) versus 9% (0–29.5) (p = 0.012), and median nighttime diastolic BP load was 35% (12.5–53.5) versus 14% (6.25–25), respectively (p = 0.019) (Table II).
Although the proportion of nondippers was higher among patients with compensatory hypertrophy compared with those without (82.4% vs 68.8%), the difference did not reach statistical significance (p=0.36) (Table II). However, mean systolic and diastolic dipping percentages were significantly higher in patients without compensatory hypertrophy (p = 0.034 and p = 0.011, respectively).
Spearman’s correlation analysis demonstrated a significant positive association between SFK length SDS and several ABP parameters. Kidney length SDS showed a moderate positive correlation with 24-hour mean systolic BP SDS (r = 0.44, p = 0.010), nighttime mean systolic BP SDS (r = 0.45, p = 0.009), nighttime mean diastolic BP SDS (r = 0.47, p = 0.006), 24-hour mean arterial pressure SDS (r = 0.41, p = 0.017), and nighttime mean MAP SDS (r = 0.45, p = 0.009). A low positive correlation was observed with daytime mean systolic BP SDS (r = 0.38, p = 0.031) (Table III).
| SFK: solitary functioning kidney, SBP: systolic blood pressure DBP: diastolic blood pressure, MAP: mean arterial blood pressure, SDS: standard deviation scores | ||
| Table III. Correlation analysis of SFK kidney length SDS and mean ambulatory BP SDS. | ||
|
|
||
|
|
|
|
| 24H-mean SBP SDS |
|
|
| 24H-mean DBP SDS |
|
|
| Day mean SBP SDS |
|
|
| Day mean DBP SDS |
|
|
| Night mean SBP SDS |
|
|
| Night mean DBP SDS |
|
|
| 24h-mean MAP SDS |
|
|
| Day mean MAP SDS |
|
|
| Night mean MAP SDS |
|
|
When subgroup analyses were performed, distinct patterns emerged between patients with and without compensatory kidney enlargement. In the agenesis subgroup, patients with compensatory enlargement showed significantly higher office systolic BP SDS values compared with those without enlargement (p = 0.001; large effect size, Cohen’s d = 1.65). In contrast, no other ABP indices differed significantly in this subgroup (Table IV).
|
Effect sizes (Cohen’s d, Hedges’ g) were calculated only for parameters showing statistically significant group differences SBP: systolic blood pressure, DBP: diastolic blood pressure, MAP: mean arterial blood pressure, SDS: standard deviation scores. Values are presented as mean ± SD or median |
||||||
| Table IV. Comparison of ambulatory blood pressure SDS values between patients with and without compensatory renal enlargement in agenesis and small kidney subgroups, and corresponding effect sizes. | ||||||
| Subgroup | Parameter |
|
|
|
|
|
| Agenesis, (n=22) |
|
|
||||
| Office SBP SDS |
|
|
|
|
|
|
| Office DBP SDS |
|
|
|
|||
| 24-h systolic BP SDS |
|
|
|
|||
| 24-h diastolic BP SDS |
|
|
|
|||
| 24-h MAP SDS |
|
|
|
|||
| Day systolic BP SDS |
|
|
|
|||
| Day diastolic BP SDS |
|
|
|
|||
| Day MAP SDS |
|
|
|
|||
| Night systolic BP SDS |
|
|
|
|||
| Night diastolic BP SDS |
|
|
|
|||
| Night MAP SDS |
|
|
|
|||
| Small atrophic kidney, (n=11) |
|
|
||||
| Office SBP SDS |
|
|
|
|||
| Office DBP SDS |
|
|
|
|||
| 24-h systolic BP SDS |
|
|
|
|
|
|
| 24-h diastolic BP SDS |
|
|
|
|||
| 24-h MAP SDS |
|
|
|
|||
| Day systolicBP SDS |
|
|
|
|||
| Day diastolic BP SDS |
|
|
|
|||
| Day MAP SDS |
|
|
|
|||
| Night systolic BP SDS |
|
|
|
|
|
|
| Night diastolic BP SDS |
|
|
|
|
|
|
| Night MAP SDS |
|
|
|
|
|
|
In the small atrophic kidney subgroup, patients with compensatory enlargement demonstrated markedly higher nocturnal BP indices, including night systolic BP SDS (p = 0.006), night diastolic BP SDS (p = 0.002), and night MAP SDS (p = 0.002), with large effect sizes (Cohen’s d ≈ 2). These findings indicate that patients with compensatory kidney enlargement tended to have significantly higher nocturnal BP indices compared with those without enlargement (Table IV). In univariate analysis, compensatory kidney enlargement was associated with an increased likelihood of hypertension, with an odds ratio (OR) of 6.22 (95% confidence interval [CI] 1.06–36.21, p = 0.042). When adjusted for age, height SDS, and weight SDS in multivariate logistic regression, compensatory enlargement remained significantly associated with elevated BP (OR 10.06, 95% CI 1.03–97.77, p = 0.047). Age demonstrated a trend toward association with hypertension in both univariate and multivariate analyses (p = 0.067 and p = 0.059, respectively), whereas height SDS and weight SDS were not significant predictors (Table V).
|
OR: odss ratio CI: confidence interval SDS: standard deviation scores * Fisher’s exact test Values are presented as mean ± SD or median (Q1–Q3) according to data distribution. |
||||||||||
| Table V. Logistic regression analysis of confounding factors related with elevated blood pressure. | ||||||||||
| Variable |
|
|
|
|||||||
|
(n=23) |
(n=10) |
|
|
|
|
|
|
|
||
| Age |
|
|
|
|
|
|
|
|
|
|
| Height SDS |
|
|
|
|
|
|
|
|
|
|
| Weight SDS |
|
|
|
|
|
|
|
|
|
|
| Compensatory enlargement* | (+) |
|
|
|
|
|
|
|
|
|
| (-) |
|
|
||||||||
Discussion
In this observational exploratory study, we evaluated ABPM profiles in children with an SFK and investigated the relationship between compensatory kidney enlargement and BP indices. A significant association between sex and compensatory kidney enlargement was observed in our cohort, with a higher proportion of females exhibiting compensatory enlargement. However, given the relatively small sample size, this finding should be interpreted with caution, as limited statistical power may influence the robustness and generalizability of the association.
In our study, 24-h systolic BP SDS, night systolic BP SDS, night MAP SDS as well as night systolic BP load and night diastolic BP load were observed to be higher in the group exhibiting compensatory growth compared to the group without a compensatory response. Subgroup analyses revealed that the pattern of BP elevation varied by the etiology of SFK. In the agenesis group, only office systolic BP SDS differed significantly according to compensatory enlargement, whereas in patients with a small atrophic kidney, the association extended to 24-hour and nocturnal ABP parameters, with large effect sizes. Subgroup analyses suggested that nocturnal BP indices tended to be higher among patients with small atrophic kidneys; however, given the limited sample size, these observations should be interpreted cautiously. In our study, a comparison of hypertension prevalence between patients with and without compensatory kidney enlargement showed a higher proportion of hypertensive cases in the compensatory enlargement group (47.1%) compared to the non-enlargement group (12.5%) but it did not reach statistical significance. These findings suggest a trend toward increased hypertension in patients with compensatory kidney enlargement; however, the small sample size warrants cautious interpretation. Although no statistically significant difference in hypertension prevalence was ultimately detected between the groups, this may reflect both the limited sample size and the diagnostic criteria used to define hypertension. In earlier studies, patients were more frequently classified as having masked or ambulatory hypertension because diagnostic definitions incorporated BP load as part of the criteria. In contrast, recent AHA guidelines no longer include BP load in the definition of ambulatory hypertension20, which may have contributed to the lower observed prevalence in the present cohort.
Previously Dursun et al. reported an increased risk of elevated BP in children with SFK without compensatory hypertrophy based on the observation of inverse correlation between kidney size SDS and 24-h MAP SDS, 24-h systolic and diastolic BP load SDS.3 However Seeman et al. could not find any significant correlation between kidney length/volume and daytime or night-time SBP/DBP in their cohort, which included MCDKs.11 Mei-Zahav et al. reported that enlargement of the remaining kidney could potentially indicate an elevation in BP and serve as a prognostic indicator.5 Our findings, in accordance with those of Mei-Zahav et al.5 led us to think that the term “compensatory hypertrophy” does not necessarily indicate that everything is functioning perfectly in the remaining kidney. While compensatory hypertrophy may be a morphological sign that the kidney is adapting to the functional nephron loss, it may not be without consequences. Many studies in the literature hypothesize that the lack of compensatory hypertrophy in SFK may be a sign of a worse prognosis in terms of preserving kidney function and the evolution of hypertension. However, it is crucial to emphasize that each person’s kidney reserve capacity and kidney characteristics are not the same. This implies that the capacity of the remaining kidney to increase single nephron GFR varies between individuals. Additionally, even among individuals born with two kidneys, there is a wide variation in nephron numbers, ranging from 500,000 to as high as 1,200,000 for each kidney. This inherent variation in nephron numbers may further contribute to the differing abilities of SFK to maintain normal kidney function and blood pressure regulation. In essence, individuals with SFK who have a higher number of nephrons in the upper range of normal and those with a lower number of nephrons in the lower range may exhibit different responses in terms of developing high BP and preserving kidney function.
In patients with an SFK, not only the presence of compensatory enlargement but also its timing should be considered. In solitary kidneys that appear in the antenatal period before 36 weeks of gestation, when nephrogenesis is completed, compensation occurs to a certain extent by nephron hyperplasia and hypertrophy in the solitary kidney, whereas in solitary kidneys that appear after the completion of nephrogenesis, compensatory growth occurs mainly by hypertrophic response.23 The presence of compensatory enlargement occurring in early childhood and even in the antenatal period before termination of nephrogenesis due to nephron hyperplasia may offer an advantage for the preservation of long-term kidney function and the attainment of normotension in certain patients with a single kidney. In our study, while no significant differences in ABP indices were observed in the renal agenesis group, the significant elevations in nocturnal BP parameters among patients with atrophic kidneys appear to support this association. However, the limited sample size necessitates cautious interpretation of these findings and represents the main limitation affecting the generalizability of the results. Studies in animal models have shown that extremely high functional kidney mass reductions (70%) in rats resulted in increased glomerular and systemic hypertension.24 The decreased surface area for filtration and limited excretion of sodium lead to extracellular volume expansion, resulting in increased cardiac output and total peripheral vascular resistance, ultimately leading to systemic hypertension. This process creates a cycle of hypertension and sclerosis, further diminishing the kidney reserve for adaptation to the decreased functional nephrons. In our study, it was observed that mean ABP were higher in patients with SFK with compensatory growth compared to the group without compensatory response and there was a positive correlation between kidney size and mainly nocturnal mean ABP indices. Logistic regression analysis suggested a potential association between compensatory enlargement and elevated BP. In multivariable models adjusted for age, height SDS, and weight SDS, compensatory enlargement appeared to be associated with elevated BP (OR 10.06, 95% CI 1.03–97.77; Table V), whereas anthropometric parameters were not significant predictors. Given the small sample size and wide confidence interval, this result should be interpreted with caution and regarded as exploratory rather than confirmatory.
Our study has several limitations. It was a single-center, cross-sectional study with a relatively small sample size, which may limit the generalizability and statistical power of the findings. Wide confidence intervals in regression analyses reflect instability of the estimates, likely due to the limited number of hypertensive cases. Therefore, these findings should be interpreted with caution. Additionally, the imbalance in sex distribution between groups may have acted as a potential confounder, as sex-related differences in kidney anthropometry and blood pressure regulation are recognized in pediatric populations.
Conclusion
To conclude, our findings suggest that compensatory hypertrophy in children with an SFK may not uniformly represent a benign adaptive response. Although kidney enlargement is generally interpreted as an indicator of adequate compensatory capacity, it may also coincide with subtle alterations in BP regulation. The observation of higher nocturnal BP indices supports the possibility that structural compensation could be accompanied by mild hemodynamic stress rather than purely reflecting healthy adaptation.
These observations should be interpreted cautiously, given the relatively small sample size and cross-sectional nature of our study. Nevertheless, they emphasize the need for careful, long-term clinical monitoring in children with SFK, as the presence of compensatory enlargement alone may not reliably indicate preserved kidney health. Future multicenter longitudinal studies with larger cohorts are warranted to better elucidate the temporal relationship between the degree and timing of compensatory kidney growth and blood pressure regulation, and to clarify the long-term implications of compensatory enlargement for kidney outcomes.
Ethical approval
The study was approved by Van Research and Education Hospital Ethics Committee (date: 21.01.2021, number: 2021/02).
Source of funding
The authors declare the study received no funding.
Conflict of interest
The authors declare that there is no conflict of interest.
References
- Rosenblum ND, Gupta IR. Disorders of kidney formation. In: Geary DF, Schaefer F, editors. Pediatric Kidney Disease. Berlin Heidelberg: Springer-Verlag; 2016: 277-303. https://doi.org/10.1007/978-3-662-52972-0_10
- Schreuder MF. Life with one kidney. Pediatr Nephrol 2018; 33: 595-604. https://doi.org/10.1007/s00467-017-3686-4
- Dursun H, Bayazit AK, Cengiz N, et al. Ambulatory blood pressure monitoring and renal functions in children with a solitary kidney. Pediatr Nephrol 2007; 22: 559-564. https://doi.org/10.1007/s00467-006-0389-7
- La Scola C, Marra G, Ammenti A, et al. Born with a solitary kidney: at risk of hypertension. Pediatr Nephrol 2020; 35: 1483-1490. https://doi.org/10.1007/s00467-020-04535-1
- Mei-Zahav M, Korzets Z, Cohen I, et al. Ambulatory blood pressure monitoring in children with a solitary kidney - a comparison between unilateral renal agenesis and uninephrectomy. Blood Press Monit 2001; 6: 263-267. https://doi.org/10.1097/00126097-200110000-00007
- Westland R, Kurvers RAJ, van Wijk JAE, Schreuder MF. Risk factors for renal injury in children with a solitary functioning kidney. Pediatrics 2013; 131: e478-e485. https://doi.org/10.1542/peds.2012-2088
- Westland R, Schreuder MF, Bökenkamp A, Spreeuwenberg MD, van Wijk JAE. Renal injury in children with a solitary functioning kidney-the KIMONO study. Nephrol Dial Transplant 2011; 26: 1533-1541. https://doi.org/10.1093/ndt/gfq844
- Westland R, Schreuder MF, van der Lof DF, et al. Ambulatory blood pressure monitoring is recommended in the clinical management of children with a solitary functioning kidney. Pediatr Nephrol 2014; 29: 2205-2211. https://doi.org/10.1007/s00467-014-2853-0
- Yel S, Günay N, Pınarbaşı AS, et al. Do children with solitary or hypofunctioning kidney have the same prevalence for masked hypertension? Pediatr Nephrol 2021; 36: 1833-1841. https://doi.org/10.1007/s00467-020-04896-7
- La Scola C, Ammenti A, Bertulli C, et al. Management of the congenital solitary kidney: consensus recommendations of the Italian Society of Pediatric Nephrology. Pediatr Nephrol 2022; 37: 2185-2207. https://doi.org/10.1007/s00467-022-05528-y
- Seeman T, John U, Bláhová K, Vondrichová H, Janda J, Misselwitz J. Ambulatory blood pressure monitoring in children with unilateral multicystic dysplastic kidney. Eur J Pediatr 2001; 160: 78-83. https://doi.org/10.1007/s004310000579
- Gurusinghe S, Palvanov A, Bittman ME, et al. Kidney volume and ambulatory blood pressure in children. J Clin Hypertens (Greenwich) 2017; 19: 498-503. https://doi.org/10.1111/jch.12954
- Neyzi O, Bundak R, Gökçay G, et al. Reference values for weight, height, head circumference, and body mass index in Turkish children. J Clin Res Pediatr Endocrinol 2015; 7: 280-293. https://doi.org/10.4274/jcrpe.2183
- Schwartz GJ, Brion LP, Spitzer A. The use of plasma creatinine concentration for estimating glomerular filtration rate in infants, children, and adolescents. Pediatr Clin North Am 1987; 34: 571-590. https://doi.org/10.1016/s0031-3955(16)36251-4
- Schwartz GJ, Haycock GB, Edelmann CM, Spitzer A. A simple estimate of glomerular filtration rate in children derived from body length and plasma creatinine. Pediatrics 1976; 58: 259-263.
- National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents. The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics 2004; 114(2 Suppl 4th Report): 555-576.
- Jean-Michel Mallion J, Pierre H, Neuder Y, Ormezzano O, Baguet JP. Validation of the AGILIS ambulatory blood pressure monitor according to the European Society of Hypertension International Protocol for validation of blood pressure measuring devices in adults. Blood Press Monit 2005; 10: 97-101. https://doi.org/10.1097/00126097-200504000-00008
- Urbina E, Alpert B, Flynn J, et al. Ambulatory blood pressure monitoring in children and adolescents: recommendations for standard assessment: a scientific statement from the American Heart Association Atherosclerosis, Hypertension, and Obesity in Youth Committee of the council on cardiovascular disease in the young and the council for high blood pressure research. Hypertension 2008; 52: 433-451. https://doi.org/10.1161/HYPERTENSIONAHA.108.190329
- Wühl E, Witte K, Soergel M, Mehls O, Schaefer F; German Working Group on Pediatric Hypertension. Distribution of 24-h ambulatory blood pressure in children: normalized reference values and role of body dimensions. J Hypertens 2002; 20: 1995-2007. https://doi.org/10.1097/00004872-200210000-00019
- Flynn JT, Urbina EM, Brady TM, et al. Ambulatory blood pressure monitoring in children and adolescents: 2022 update: a scientific statement from the American Heart Association. Hypertension 2022; 79: e114-e124. https://doi.org/10.1161/HYP.0000000000000215
- Obrycki Ł, Sarnecki J, Lichosik M, et al. Kidney length normative values - new percentiles by age and body surface area in Central European children and adolescents. Pediatr Nephrol 2023; 38: 1187-1193. https://doi.org/10.1007/s00467-022-05667-2
- Obrycki Ł, Sarnecki J, Lichosik M, et al. Kidney length normative values in children aged 0-19 years - a multicenter study. Pediatr Nephrol 2022; 37: 1075-1085. https://doi.org/10.1007/s00467-021-05303-5
- Davidovits M, Cleper R, Eizenberg N, Hocherman O, Mashiach R. Outcomes of prenatally diagnosed solitary functioning kidney during early life. J Perinatol 2017; 37: 1325-1329. https://doi.org/10.1038/jp.2017.143
- Brenner BM, Garcia DL, Anderson S. Glomeruli and blood pressure. Less of one, more the other? Am J Hypertens 1988; 1: 335-347. https://doi.org/10.1093/ajh/1.4.335
Copyright and license
Copyright © 2026 The Author(s). This is an open access article distributed under the Creative Commons Attribution License (CC BY), which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is properly cited.









