
Graphical Abstract
Abstract
Background. Unlike polythelia, which is typically identified at birth by the presence of an areola or nipple, accessory axillary breast tissue is rarely observed in children and adolescents. Nevertheless, it can affect this age group and should be considered in the differential diagnosis of an axillary mass.
Case Presentation. A 15-year-old girl with a diagnosed prolactinoma, receiving cabergoline treatment, presented with a week’s history of tender, bilateral axillary masses. Ultrasonographic evaluation and subsequent surgical excision confirmed the diagnosis of bilateral accessory axillary breast tissue. To the best of our knowledge, this is the first reported case of co-existing bilateral accessory axillary breast tissue and prolactinoma in an adolescent girl.
Conclusion. This case highlights the importance of thorough physical examination in adolescents with prolactinomas. Accessory breast tissue may become more prominent during puberty or in hyperprolactinemic states, and it may be misdiagnosed. Recognizing this rare occurrence is key to avoiding unnecessary investigations or interventions.
Keywords: accessory breast tissue, polymastia, prolactinoma
| Table I. Classification of accessory breast tissue as proposed by Kajava in19153. | ||
| Clinical category | Alternative name | Definition |
| Class I | Polymastia | A complete breast including glandular tissue, nipple, and areola |
| Class II | Polymastia, supernumerary breast without areola | Only glandular tissue and nipple, without areola |
| Class III | Polymastia, supernumerary breast without nipple | Only glandular tissue and areola, without nipple |
| Class IV | Mamma aberrata | Glandular tissue only |
| Class V | Pseudomamma | Nipple and areola but without glandular tissue (replaced by fat) |
| Class VI | Polythelia | Nipple only |
| Class VII | Polythelia areolaris | Areola only |
| Class VIII | Polythelia pilosa | Patch of hair only |
Introduction
Accessory breast tissue consists of normal breast tissue located outside the breast. This ectopic breast tissue can develop anywhere along the mammary ridges due to incomplete involution (the ‘milk line’). It includes a range of conditions characterized by the presence of glandular tissue (polymastia), supernumerary nipples without breast tissue (polythelia), areolas, or combinations of these features.1 Kajava proposed a classification system in 1915 that remains widely used today (Table I). Polythelia is most often found on the chest, upper abdomen, or just below the normally positioned breast, whereas the most common site of accessory breast tissue is the axilla, where it may occur unilaterally or bilaterally.2 Some forms of accessory breast tissue are present at birth, whereas others may become apparent later in life during periods of hormonal change such as pregnancy or menstruation.3 It affects between 0.4% and 6.0% of the general population.3 The diagnosis of accessory axillary breast tissue is rare in children and adolescents, with only a few detailed cases in these groups reported in the literature.3-5
Prolactin (PRL) plays a key role in the development of mammary glands within breast tissue and in milk production. Prolactinomas are the most common organic cause of hyperprolactinemia and represent the most prevalent type of pituitary adenoma in children and adolescents.6 The clinical manifestations of prolactinomas vary according to the patient’s sex and age at onset, as well as tumor size. Where emergency surgery is not indicated, the first-line treatment for prolactinoma is dopamine agonists, which both normalize PRL levels and reduce tumor size.7
Hyperprolactinemia, particularly when caused by prolactinomas, can stimulate mammary gland development and milk production. However, only a few well-documented cases of bilateral accessory breast tissue in adults with prolactinoma have been reported in the literature.8 Hyperprolactinemia, particularly when caused by prolactinomas, can stimulate mammary gland development and milk production. Existing evidence is limited to isolated adult case reports, and prior publications have not conclusively clarified whether prolactin exerts a direct proliferative effect on accessory axillary breast tissue.8,9 The absence of pediatric data and the lack of mechanistic evidence in adult studies underscore the current gaps in the literature.Here, we describe a case involving an adolescent girl diagnosed with a prolactinoma and bilateral axillary accessory breasts, with the aim of providing clinicians with additional diagnostic and treatment experience. Reports of accessory axillary breast tissue in the pediatric population are scarce, and, to the best of our knowledge, coexistence with prolactinoma has not been previously described in an adolescent.
Case Presentation
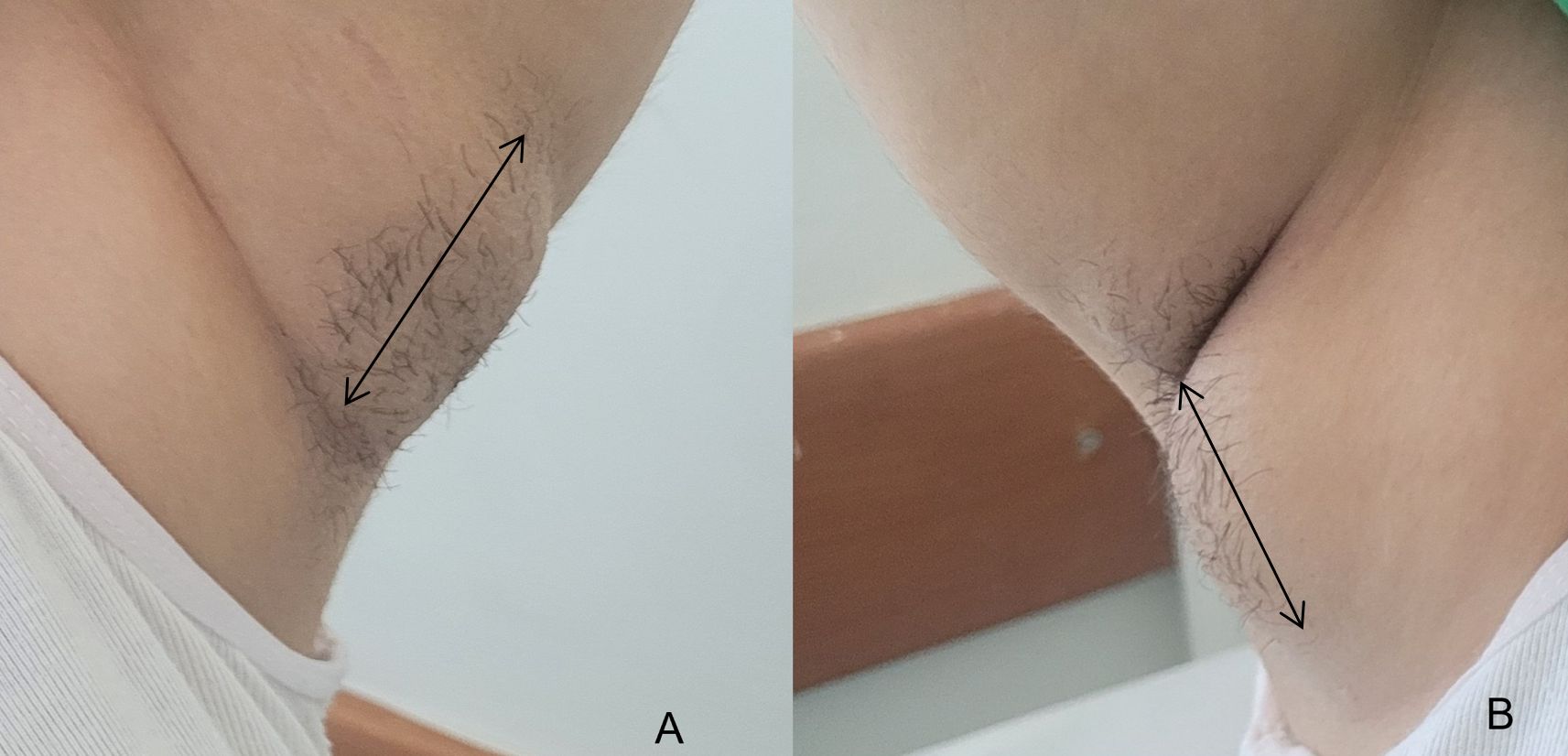
A 15-year-old girl presented with heavy menstrual bleeding. The patient experienced menarche at the age of 12. During the first year following menarche, her menstrual cycles occurred approximately every two months, after which they became regular on a monthly basis. The amount of menstrual bleeding had not previously been excessive, typically not exceeding four sanitary pads per day. On laboratory evaluation, her hemoglobin was 8.6 g/dL (normal [N]: 11.7-15), ferritin 3.9 µg/L (N: 12-140), luteinizing hormone (LH) 2.8 IU/L (N: 2.4-12.6), follicle-stimulating hormone (FSH) 7.2 IU/L (N: 3.5-12.5), estradiol (E2) 32.2 ng/L (N: 22-341), and total testosterone 30 ng/dL (N: 20-38). Her PRL level was 78 ng/mL (N: 5-20 ng/ml) in tests conducted prior to the initiation of combined oral contraceptive treatment. Magnetic resonance imaging (MRI) revealed a pituitary microadenoma measuring 7.5 × 6.0 × 7.0 mm. Evaluation of the other pituitary hormones revealed an adrenocorticotropic hormone (ACTH) level of 27.5 pg/mL (N: 7.2-63), a cortisol level of 11.3 µg/dL (N: 4.8-19), and an insulin-like growth factor (IGF)-1 level of 229 ng/mL (N: 151-485). According to her medical history, other than asthma treatment administered prior to puberty, she had no exposure to medications associated with hyperprolactinemia or abnormal uterine bleeding. Following acute management of heavy menstrual bleeding, the patient was monitored while receiving cabergoline 0.5 mg/week. The PRL level normalized (7 ng/mL) within the first month, with an MRI at six months showing initial adenoma shrinkage, and one-year follow-up imaging confirming a reduction in size to 3.8 × 2.7 mm. A PRL level below 20 ng/mL was maintained. At an outpatient visit, the patient reported bilateral axillary swelling that had developed over the preceding week, following a month of irregular medication use. This episode occurred during the first year of prolactinoma treatment, when her PRL level had increased to 29 ng/mL. On examination, painful swellings were present beneath both axillae, without erythema, ulceration, or palpable fluctuation (Fig. 1). No galactorrhea was observed. She had no history of tuberculosis, cat-scratch disease, or other systemic infection. There was no evidence of pathological lymphadenopathy or organomegaly. Laboratory tests showed a PRL level of 28 ng/mL and a negative β-hCG result. At the time the axillary swelling developed, the patient was menstruating. Gonadotropin levels (LH and FSH) were not measured during this episode. No palpable masses were found in either breast. Bilateral mammary gland tissue was detected on axillary ultrasound, with the accessory tissue more prominent on the right side. The accessory breast observed in this patient corresponded to Class IV in Kajava’s classification system (Table I). There was no reported family history of a similar condition.
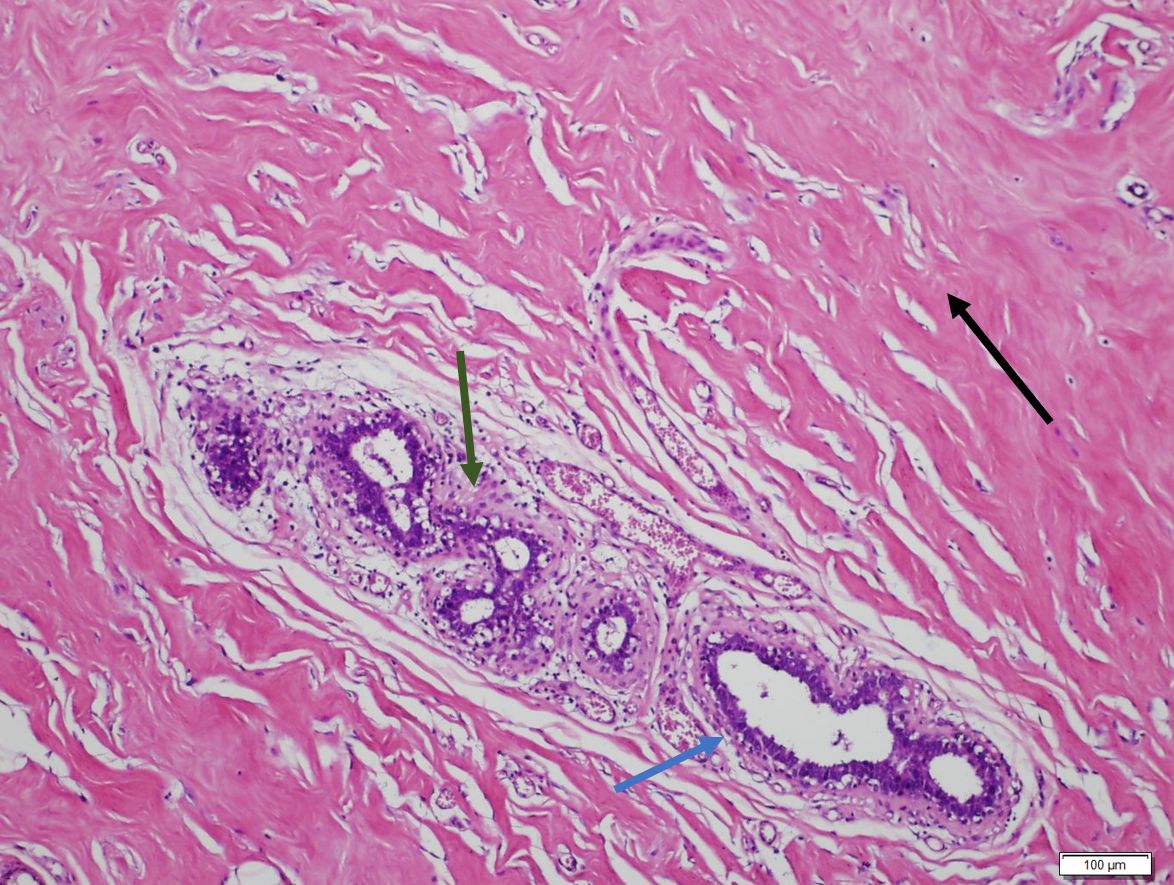
The cabergoline dose was increased to 1 mg/week. Echocardiography was normal. An abdominal ultrasound performed to check for associated anomalies revealed no abnormalities in the kidneys or other organs. The patient was referred to surgery with a pre-diagnosis of bilateral axillary breast tissue, and the pediatric surgeon recommended elective excision (Fig. 2). Histopathological findings revealed normal mammary tissue without atypia in the bilateral accessory breast tissues, confirming the diagnosis of bilateral accessory axillary breast tissue (Fig. 3). The incision healed well, and no recurrence was observed during the 3-month follow-up period. Written informed consent for publication of the case details and accompanying images was obtained from the patient and her legal guardian.

Discussion
To the best of our knowledge, this is the first reported adolescent patient with co-existing bilateral accessory axillary breast tissue and prolactinoma. Although numerous cases of accessory axillary breast tissue have been reported in adults, only a few have been described in children and adolescents.3,5,10 In one case series of 11 adolescents with axillary accessory breast tissue, the youngest patient was 13 years old.3 Another case report described a 9-year-old prepubertal girl with bilateral axillary accessory breasts.5
The relatively small number of reported cases in children may be due to the condition going unnoticedeither because accessory axillary breast tissue only becomes apparent and symptomatic after hormonal stimulation, or because the patient’s body shape obscures it. Hormonal changes (e.g. menstruation, pregnancy, and lactation) can cause the masses to become tender and fluctuate in size.11
In this case, no complaints were reported at the time of prolactinoma diagnosis, and no axillary mass was palpable during the initial physical examination. The findings only became apparent during the menstrual cycle in the first year of treatment. This situation can be explained as follows. Hyperprolactinemia can lead to menstrual irregularity, estrogen deficiency, and testosterone deficiency. 7In our patient, treatment with cabergoline improved gonadal function, and the accessory breast tissue may have become more prominent as estrogen levels returned to normal. PRL promotes the growth of mammary alveoli and stimulates breast alveolar epithelial cells to synthesize milk components 6. At the same time, the effects of PRL on breast tissue may render accessory breast tissue more noticeable. Our case is noteworthy due to the delayed presentation of accessory breast tissue following a period of irregular cabergoline use, despite the patient having previously achieved target PRL levels. A plausible explanation is that normalization of PRL may have permitted reactivation of the hypothalamic–pituitary–gonadal axis, leading to increased gonadotropin secretion; however, the exact underlying mechanism remains unclear. Accessory breast tissue originates during embryological development and typically becomes clinically apparent during periods of hormonal fluctuation such as puberty, menstruation, pregnancy, or lactation.3 In this patient, the transient rise in PRL or associated hormonal imbalances may have triggered an earlier or more pronounced manifestation of the accessory breast tissue.
Ultrasonography is the recommended imaging method for children and adolescents suspected of having accessory breast tissue. However, histopathological examination is required to confirm the diagnosis and to demonstrate histological features characteristic of normal breast tissue.2,3
Polythelia often does not require surgery. By contrast, surgical excision of axillary breast tissue enables confirmation of the diagnosis, relief of pain, and improvement of cosmetic appearance.12,13Accessory breast tissue is subject to the same benign and malignant pathologies as normal breast tissue, including pain, swelling, lactation, mastopathy, fibroadenoma, fibrocystic change, and carcinoma.14-16
Accessory breasts can be inherited as an autosomal dominant trait with incomplete penetrance, although they are more often sporadic.3 In our case, there was no family history of accessory axillary breast tissue. The literature describes familial incidence, as well as associations with cardiovascular or renal anomalies and trisomy 21, but none of these anomalies were present in our patient.10
The classical syndrome is characterized by cyclic pain during menstruation, accompanied by symptoms such as swelling, tenderness, restricted shoulder mobility, and irritation from clothing. 10
Possible differential diagnoses include lymphadenopathy, hidradenitis suppurativa, lipoma, malignancy, sebaceous cyst, plexiform neurofibroma, neuroma, follicular cyst, slack skin with granulomatous inflammation, and vascular malformation.10-12,17
Ultrasonography is the initial diagnostic tool, typically revealing hypoechoic breast tissue similar to orthotopic tissue. Bilateral ultrasonography is recommended to rule out contralateral involvement. Histopathological examination is required to confirm the diagnosis.2 The risk of incision-site infection and recurrence can be reduced by complete excision of the lesion along with the surrounding skin.3
However, there is some controversy in the literature regarding the optimal timing of surgery. Many authors argue that the best time is before pregnancy because the reoperation rate is lower and patients are more satisfied when the procedure is carried out at a young age.18Monitoring and reducing serum PRL levels may lessen disease severity, shorten the treatment period, lower the risk of recurrence, and help prevent or manage endocrine disorders associated with hyperprolactinemia.
Children and adolescents with a supernumerary nipple or areola should be made aware of the possibility of underlying breast tissue. Consequently, follow-up is recommended until the end of puberty.3Although accessory breasts are often asymptomatic, they may cause anxiety, cosmetic concerns, pain, and restricted arm movement. According to the literature, excision of accessory axillary breast tissue has also been associated with notable adverse effects.3,4 In the present case bilateral surgical excision was performed because of persistent pain, cosmetic concerns, and the need for definitive histopathological confirmation. In the context of the underlying hyperprolactinemic state and the bilateral symptomatic presentation, surgical management was deemed the most appropriate approach to ensure symptom relief and diagnostic certainty.
Gonadotropin levels (LH and FSH) were not assessed at the time of detection of bilateral axillary breast tissue; although such measurements could have provided additional insight into the hormonal milieu, they were not obtained at that time. An important limitation of this case is the relatively short postoperative follow-up period of three months, which is insufficient to thoroughly assess recurrence risk or long-term cosmetic outcomes. An extended follow-up would be necessary to better characterize the long-term course and overall surgical success.
Conclusion
We have presented what we believe to be the first case report of the co-existence of accessory axillary breast tissue and prolactinoma in an adolescent girl. Axillary accessory breast tissue should be considered in the differential diagnosis of axillary masses in pediatric patients. Symptoms may arise before pregnancy and prior to the end of puberty. The most common are axillary swelling and cyclic pain coinciding with menstruation. Bilateral ultrasonography is widely recommended for diagnosis. Surgical management is safe and effective in children and adolescents. This case contributes to the limited literature on the association between prolactinomas and bilateral axillary accessory breast tissue in adolescence.
Ethical approval
Written informed consent was obtained from the patient’s guardian for the publication of the case details and images.
Source of funding
The authors declare the study received no funding.
Conflict of interest
The authors declare that there is no conflict of interest.
References
- Burdick AE, Thomas KA, Welsh E, Powell J, Elgart GW. Axillary polymastia. J Am Acad Dermatol 2003; 49: 1154-1156. https://doi.org/10.1016/s0190-9622(03)00467-5
- DeFilippis EM, Arleo EK. The ABCs of accessory breast tissue: basic information every radiologist should know. AJR Am J Roentgenol 2014; 202: 1157-1162. https://doi.org/10.2214/AJR.13.10930
- De la Torre M, Lorca-García C, de Tomás E, Berenguer B. Axillary ectopic breast tissue in the adolescent. Pediatr Surg Int 2022; 38: 1445-1451. https://doi.org/10.1007/s00383-022-05184-1
- Sadove AM, van Aalst JA. Congenital and acquired pediatric breast anomalies: a review of 20 years’ experience. Plast Reconstr Surg 2005; 115: 1039-1050. https://doi.org/10.1097/01.prs.0000154214.99641.72
- Class MM, McCoy K, Melin AA, Hafeez F, Abidi N, Krakowski AC. Bilateral accessory axillary breast tissue in a premenarchal female. Pediatr Dermatol 2024; 41: 704-706. https://doi.org/10.1111/pde.15565
- Kontbay T, Şıklar Z, Özsu E, et al. Hyperprolactinemia in children and adolescents and longterm follow-up results of prolactinoma cases: a single-centre experience. Turk J Pediatr 2022; 64: 892-899. https://doi.org/10.24953/turkjped.2021.4639
- Wong A, Eloy JA, Couldwell WT, Liu JK. Update on prolactinomas. Part 1: clinical manifestations and diagnostic challenges. J Clin Neurosci 2015; 22: 1562-1567. https://doi.org/10.1016/j.jocn.2015.03.058
- Liu J, Cong H, Chen X, et al. Duct ectasia of bilateral accessory breast associatedwith pituitary microadenoma: a case report and literature review. Emergency and Critical Care Medicine 2023; 3: 36-40. https://doi.org/10.1097/EC9.0000000000000079
- Lages RB, Neto TRG, Cabral RFB, Cabral RFB, Araujo RC, Vieira SC. Fibroadenoma of the axilla in a patient with macroprolactinoma. Journal of Medical Cases 2011; 2: 279-283. https://doi.org/10.4021/jmc384w
- Kogut M, Bidier M, Enk A, Hassel JC. Axillary accessory breast tissue-case report and review of literature. J Dtsch Dermatol Ges 2014; 12: 499-500. https://doi.org/10.1111/ddg.12285
- Ghosn SH, Khatri KA, Bhawan J. Bilateral aberrant axillary breast tissue mimicking lipomas: report of a case and review of the literature. J Cutan Pathol 2007; 34(Suppl 1): 9-13. https://doi.org/10.1111/j.1600-0560.2006.00713.x
- van Aalst JA, Sadove AM. Treatment of pediatric breast problems. Clin Plast Surg 2005; 32: 65-78. https://doi.org/10.1016/j.cps.2004.08.005
- Famá F, Cicciú M, Sindoni A, et al. Prevalence of ectopic breast tissue and tumor: a 20-year single center experience. Clin Breast Cancer 2016; 16: e107-e112. https://doi.org/10.1016/j.clbc.2016.03.004
- Patel RV, Govani D, Patel R, Bhayani B. Adolescent right axillary accessory breast with galactorrhoea. BMJ Case Rep 2014; 2014: bcr2014204215. https://doi.org/10.1136/bcr-2014-204215
- Yefter ET, Shibiru YA. Fibroadenoma in axillary accessory breast tissue: a case report. J Med Case Rep 2022; 16: 341. https://doi.org/10.1186/s13256-022-03540-2
- Sikdar O, Roy M, Al-Ishaq Z, Shinde V, Sircar T. A rare case of primary carcinoma of axillary accessory breast tissue. J Surg Case Rep 2021; 2021: rjab473. https://doi.org/10.1093/jscr/rjab473
- Jordan K, Laumann A, Conrad S, Medenica M. Axillary mass in a 20-year-old woman. Diagnosis: axillary accessory breast tissue. Arch Dermatol 2001; 137: 1367-1372.
- Lee SR, Lee SG, Byun GY, Kim MJ, Koo BH. Axillary accessory breast: optimal time for operation. Aesthetic Plast Surg 2018; 42: 1231-1243. https://doi.org/10.1007/s00266-018-1128-8
Copyright and license
Copyright © 2026 The Author(s). This is an open access article distributed under the Creative Commons Attribution License (CC BY), which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is properly cited.









