
Abstract
Background. This case report describes a rare presentation of rippling muscle disease (RMD) due to a pathogenic CAV3 variant, manifesting with myocarditis-like cardiac involvement in an adolescent patient. To the best of our knowledge, this represents an exceedingly rare pediatric case of RMD associated with clinically significant cardiac findings.
Case Presentation. A previously healthy 15-year-old male adolescent presented with vomiting and markedly elevated creatine kinase and troponin levels, raising suspicion of acute myocarditis. Cardiac magnetic resonance imaging (MRI) demonstrated non-ischemic myocardial fibrosis, and genetic testing identified a pathogenic de novo variant in the CAV3 gene consistent with rippling muscle disease.
Conclusions. This case highlights the potential for myocarditis-like cardiac involvement in caveolin-3–related rippling muscle disease and underscores the importance of considering underlying genetic myopathies in adolescents presenting with unexplained elevations of serum creatine kinase (hyperCKemia) and cardiac biomarkers.
Keywords: Rippling muscle disease, pediatric cardiomyopathy, caveolin-3 (CAV3) mutation, non-ischemic myocardial fibrosis
Introduction
Rippling muscle disease (RMD) is a myopathy caused by pathogenic variants in the CAV3 gene encoding caveolin-3, typically inherited in an autosomal dominant manner, although rare autosomal recessive cases have also been reported.1 The clinical spectrum ranges from asymptomatic elevation of serum creatine kinase (hyperCKemia) to muscle stiffness, mechanically induced muscle rippling, exercise intolerance, and limb-girdle muscular dystrophy phenotypes.1 Although cardiac involvement has been described in caveolinopathies2-4, pediatric cases remain limited.2
In the acute setting, adolescents presenting with chest pain or elevated troponin levels are frequently evaluated for myocarditis. However, when CK elevation is disproportionately high or persists despite supportive treatment, alternative diagnoses such as genetic myopathies must be considered.
Here, we report a previously healthy adolescent with suspected myocarditis and persistent hyperCKemia who was ultimately diagnosed with rippling muscle disease due to a pathogenic CAV3 variant, with cardiac magnetic resonance imaging revealing non-ischemic myocardial fibrosis.
Case Presentation
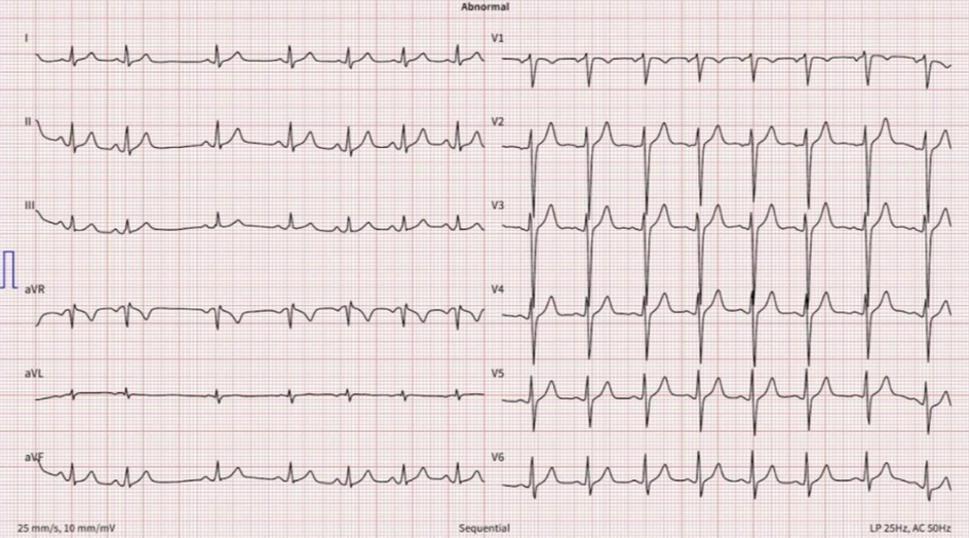
A previously healthy 15-year-old male adolescent presented to the emergency department with vomiting. He denied fever, myalgia, recent upper respiratory symptoms, exercise intolerance, or supplement use. Physical examination revealed full muscle strength (5/5) in all extremities, with mild hypertrophy of the lower-limb muscles, particularly in the calf region. The patient’s weight was 105 kg (>97th percentile) and height was 165 cm (approximately 10th–25th percentile), with a body mass index of 38.6 kg/m² (>97th percentile for age and sex), consistent with severe obesity. Mild calf hypertrophy was evident on both anterior and lateral views (Fig. 1 and Fig. 2). The remainder of the systemic examination was unremarkable. Initial laboratory investigations demonstrated markedly elevated creatine kinase (CK, 8,612 U/L; reference range: <270 U/L) and troponin T (65 ng/L; reference range: 0–14 ng/L). His past medical history was unremarkable. There was no parental consanguinity and no family history of neuromuscular or cardiac disease. The electrocardiogram (ECG) demonstrated normal sinus rhythm with sinus arrhythmia, without conduction abnormalities or ectopy (Fig. 3). Transthoracic echocardiography showed prominent left ventricular trabeculations, raising suspicion for left ventricular noncompaction cardiomyopathy. The patient was admitted with a provisional diagnosis of acute myocarditis and was started on intravenous hydration and supportive management. Twenty-four-hour Holter monitoring revealed no arrhythmias.


During hospitalization, CK levels continued to rise, peaking at 32,448 U/L. By day 10 of treatment, CK decreased to 3,642 U/L and troponin T to 40 ng/L, and the patient was subsequently discharged.
Metabolic evaluation, including tandem mass spectrometry, plasma amino acid analysis, urine organic acid analysis, serum lactate, and ammonia levels, yielded normal results, thereby excluding relatively more common inborn errors of metabolism, including fatty acid oxidation defects, mitochondrial disorders, and organic acidemias. Targeted genetic testing panels for Duchenne muscular dystrophy and glycogen storage diseases were negative. Whole exome sequencing revealed a heterozygous variant c.80G>A, p.(Arg27Gln) in the CAV3 (NM_033337.3) gene. This variant has been previously reported and characterized as pathogenic in the literature.5 The variant was confirmed by Sanger sequencing. Sanger sequencing also showed that this change was not present in the parents, thus confirming a de novo occurrence in this case.
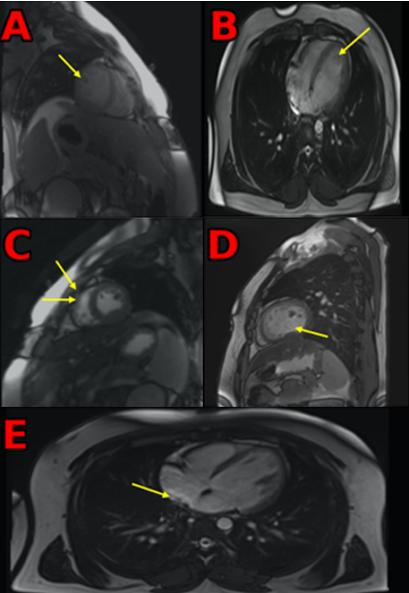
The NC/C ratio was defined as the ratio of the thickness of the noncompacted myocardial layer to the compacted myocardial layer, measured at end-diastole. An NC/C ratio >2.3 was considered diagnostic for left ventricular noncompaction. Cardiac magnetic resonance imaging demonstrated increased left ventricular trabeculation with an NC/C ratio of 11.6/2.6 = 4.46, indicating prominent trabeculation. No myocardial edema was identified on T2-weighted or T2-mapping sequences. Late gadolinium enhancement revealed subepicardial to mid-myocardial non-ischemic fibrosis involving the basal inferolateral and inferoseptal walls, as well as the mid-inferior and mid-inferoseptal segments (Fig. 4). Electromyography performed using a myasthenia protocol was unremarkable.
Based on the integration of clinical, biochemical, genetic, and imaging findings, the patient was diagnosed with caveolin-3–related rippling muscle disease with subclinical cardiac involvement. During an 18-month follow-up period, our patient remained clinically stable, with no evidence of arrhythmias or deterioration in cardiac function. Written informed consent was obtained from the patient’s parents for publication of this case report and accompanying images.
Discussion
Rippling muscle disease (RMD) is a rare caveolinopathy caused by pathogenic variants in CAV3, which encodes the muscle-specific scaffolding protein caveolin-3. Although classically considered a skeletal-muscle disorder, caveolin-3 is also expressed in cardiomyocytes; consequently, cardiac involvement—including cardiomyopathy and arrhythmias—has been described across the caveolinopathy spectrum, with CAV3 mutations also reported in patients with long QT syndrome, sudden infant death syndrome, and hypertrophic cardiomyopathy.2-4 Our adolescent patient had the pathogenic c.80G>A, p.(Arg27Gln) variant and presented with marked hyperCKemia and myocarditis-like biomarker elevation. Despite a normal EMG, which has been repeatedly reported in CAV3-related disorders and can delay diagnosis, cardiac MRI (CMR) demonstrated non-ischemic late gadolinium enhancement (LGE) consistent with myocardial fibrosis. These findings expand the pediatric phenotypic spectrum of caveolin-3–related disease, in which skeletal and cardiac phenotypes may occur together or separately, and the same mutation may produce variable expressivity.6
Mechanistically, caveolin-3 organizes caveolae and key signaling microdomains in the sarcolemma. Experimental work indicates that perturbations in caveolin-3 levels alter cardioprotective signaling and can facilitate ventricular dysfunction and arrhythmogenesis, providing a plausible substrate for the fibrosis observed on CMR.7 Clinically, non-ischemic LGE in pediatric myopathies is increasingly recognized as a marker of early myocardial disease and adverse remodeling; while most data derive from Duchenne dystrophy cohorts, the principle that LGE heralds cardiomyopathy progression is likely generalizable to caveolinopathies and supports longitudinal surveillance.8
An important differential in our case is prior myocarditis, given the elevated troponin and the subepicardial/mid-myocardial LGE pattern—features that can follow viral myocarditis. However, the coexistence of a pathogenic CAV3 variant and skeletal-muscle phenotype argues for overlapping etiologies: (i) CAV3-related myocardial vulnerability with early fibrosis, and/or (ii) a myocarditis episode unmasking an underlying caveolinopathy. Similar coexistence and phenotype variability have been emphasized previously, with calls for systematic cardiac screening in patients with CAV3 variants.8
The trabeculation increase (NC/C 4.46) observed in this patient raises the question of left ventricular noncompaction (LVNC). While LVNC can occur in childhood and often has a genetic basis, its relationship to caveolinopathies is not fully defined and requires cautious interpretation alongside clinical context and family studies.9 Regardless of taxonomy, our findings justify structured pediatric cardiac follow-up in CAV3-positive patients, including periodic ECG/Holter monitoring and interval CMR when feasible, given potential risks of conduction disease, ventricular arrhythmias, and progressive cardiomyopathy.10
Pathogenic variants in CAVIN1 cause Congenital Generalized Lipodystrophy type 4, characterized by muscle rippling, elevated creatine kinase levels, arrhythmias, prominent endocrinological abnormalities (e.g., insulin resistance, hyperinsulinism, acanthosis nigricans), and gastrointestinal involvement, reflecting a multisystem disorder unlike CAV3-related Rippling Muscle Disease 2.
Monoallelic variants in CAV3 are associated with a broad phenotypic spectrum beyond Rippling Muscle Disease 2, including Familial Hypertrophic Cardiomyopathy 1, isolated hyperCKemia, Long QT Syndrome 9, and Tateyama-type distal myopathy. The variant identified in our patient has previously been reported in cases with neurological involvement, particularly distal myopathy.11,12 Additionally, CAV3 variants have been linked to cardiovascular disorders such as long QT syndrome, atrial standstill, sudden infant death, and cardiomyopathy.10 Given the role of caveolin-3 in cardioprotective signaling, comprehensive cardiac evaluation and neurological follow-up are recommended.
This case highlights the importance of considering caveolinopathies in pediatric patients presenting with unexplained hyperCKemia and myocardial injury markers, even when myocarditis is initially suspected and neuromuscular symptoms are absent. Clinicians should be aware that CK levels should be evaluated in patients presenting with elevated troponin levels and suspected myocarditis, as disproportionately high CK values may indicate an underlying genetic myopathy. The coexistence of a pathogenic CAV3 mutation and non-ischemic myocardial fibrosis on CMR expands the phenotypic spectrum of caveolin-3–related myopathies and underscores the need for early recognition, genetic counseling, and cardiac surveillance. To our knowledge, this represents one of the first reported pediatric cases from Türkiye, further expanding the limited literature on cardiac involvement in CAV3-related disease.
Ethical approval
Not applicable. Written informed consent was obtained from the patient’s parents for publication of this case report and accompanying images.
Source of funding
The authors declare the study received no funding.
Conflict of interest
The authors declare that there is no conflict of interest.
References
- Kubisch C, Ketelsen UP, Goebel I, Omran H. Autosomal recessive rippling muscle disease with homozygous CAV3 mutations. Ann Neurol 2005; 57: 303-304. https://doi.org/10.1002/ana.20350
- Cronk LB, Ye B, Kaku T, et al. Novel mechanism for sudden infant death syndrome: persistent late sodium current secondary to mutations in caveolin-3. Heart Rhythm 2007; 4: 161-166. https://doi.org/10.1016/j.hrthm.2006.11.030
- Hayashi T, Arimura T, Ueda K, et al. Identification and functional analysis of a caveolin-3 mutation associated with familial hypertrophic cardiomyopathy. Biochem Biophys Res Commun 2004; 313: 178-184. https://doi.org/10.1016/j.bbrc.2003.11.101
- Vatta M, Ackerman MJ, Ye B, et al. Mutant caveolin-3 induces persistent late sodium current and is associated with long-QT syndrome. Circulation 2006; 114: 2104-2112. https://doi.org/10.1161/CIRCULATIONAHA.106.635268
- Nie H, Wu X, Lyu J, Zhu J, Tan D. Clinical and genetic study of a Chinese family affected with caveolinopathies. Zhonghua Yi Xue Yi Chuan Xue Za Zhi 2017; 34: 650-653. https://doi.org/10.3760/cma.j.issn.1003-9406.2017.05.006
- Catteruccia M, Sanna T, Santorelli FM, et al. Rippling muscle disease and cardiomyopathy associated with a mutation in the CAV3 gene. Neuromuscul Disord 2009; 19: 779-783. https://doi.org/10.1016/j.nmd.2009.08.015
- Tsutsumi YM, Horikawa YT, Jennings MM, et al. Cardiac-specific overexpression of caveolin-3 induces endogenous cardiac protection by mimicking ischemic preconditioning. Circulation 2008; 118: 1979-1988. https://doi.org/10.1161/CIRCULATIONAHA.108.788331
- Hor KN, Taylor MD, Al-Khalidi HR, et al. Prevalence and distribution of late gadolinium enhancement in a large population of patients with Duchenne muscular dystrophy: effect of age and left ventricular systolic function. J Cardiovasc Magn Reson 2013; 15: 107. https://doi.org/10.1186/1532-429X-15-107
- Lehman MB, Orgil BO, Guerrier K, et al. Left ventricular noncompaction cardiomyopathy in children: a focus on genetic and molecular mechanisms. Rev Cardiovasc Med 2025; 26: 39044. https://doi.org/10.31083/RCM39044
- He M, Qiu J, Wang Y, Bai Y, Chen G. Caveolin-3 and arrhythmias: insights into the molecular mechanisms. J Clin Med 2022; 11: 1595. https://doi.org/10.3390/jcm11061595
- Fulizio L, Nascimbeni AC, Fanin M, et al. Molecular and muscle pathology in a series of caveolinopathy patients. Hum Mutat 2005; 25: 82-89. https://doi.org/10.1002/humu.20119
- González-Pérez P, Gallano P, González-Quereda L, et al. Phenotypic variability in a Spanish family with a Caveolin-3 mutation. J Neurol Sci 2009; 276: 95-98. https://doi.org/10.1016/j.jns.2008.09.009
Copyright and license
Copyright © 2026 The Author(s). This is an open access article distributed under the Creative Commons Attribution License (CC BY), which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is properly cited.









