
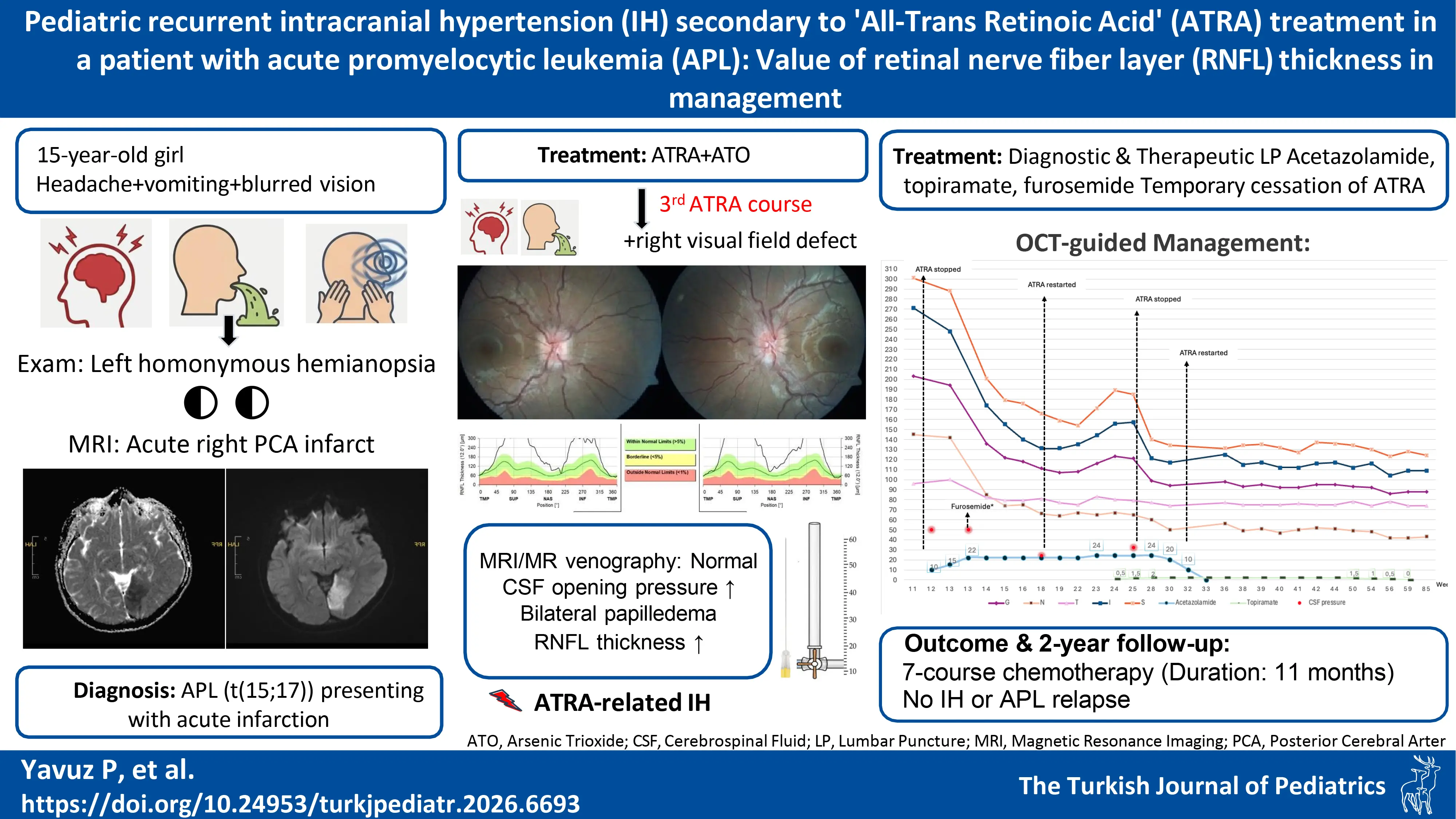
Graphical Abstract
Abstract
Background. All-trans retinoic acid (ATRA) is an essential agent in the treatment of acute promyelocytic leukemia (APL). However, careful monitoring is required due to its potential side effects, particularly intracranial hypertension (IH).
Case Presentation. Here, we report a 15-year-old girl who presented with headache, blurred vision, vomiting, and was found to have left homonymous hemianopsia and an acute cerebral infarct. Etiological investigations revealed acute promyelocytic leukemia and treatment with ATRA was initiated. However, this treatment was complicated by repetitive episodes of IH, which improved with discontinuation of ATRA but recurred whenever reinitiation was attempted. Despite this side effect, the patient was able to complete the planned ATRA course under medical treatment of IH, guided by retinal nerve fiber layer (RNFL) thickness measured using optical coherence tomography (OCT).
Conclusions. Changes in papilledema were detected on OCT earlier than on clinical examination. This case illustrates the reversibility of IH secondary to ATRA therapy, the feasibility of completing ATRA treatment despite the side effect of IH, the importance of medical treatment for IH in combination with appropriate dose adjustments, and the accuracy and convenience of RNFL thickness as a biomarker for treatment efficiency. Managing IH in the context of a chronic systemic disorder requires a collaborative approach, close follow-up, and individualized management.
Keywords: acute promyelocytic leukemia, ATRA, intracranial hypertension, papilledema, retinal nerve fiber layer thickness
Introduction
All-trans retinoic acid (ATRA), a metabolite of vitamin A, has been shown to significantly improve outcomes for patients with acute promyelocytic leukemia (APL), in which the prognosis was poor before the introduction of this agent.1 APL’s response rate to ATRA is high, but of limited duration; its combination with arsenic trioxide (ATO) and chemotherapy prolongs remission and results in a 10-year overall survival rate of over 85%.1 ATRA’s potential side effects include intracranial hypertension (IH), and pseudotumor cerebri syndrome, occurring in up to 13% of pediatric and 2-7% of adult patients.2 This can lead to interruption of treatment. Studies have reported that treatment can be carried out by discontinuing ATRA and restarting it at lower doses.3
Early diagnosis and appropriate management of IH secondary to ATRA are critical for the success of treatment in APL. IH can present with headache, visual field defects, and cranial nerve palsies. A definitive diagnosis is made by measuring intracranial pressure via lumbar puncture (LP).4 The IH diagnostic criteria, which provide a standardized framework for diagnosis, are provided in Supplementary Table I.4 However, LP carries a certain risk in APL patients due to their tendency for bleeding; therefore, clinical follow-up of symptoms and opthalmological examination findings are important in practice, although the assessment of the fundus can be challenging in young children. Noninvasive imaging methods such as ocular ultrasound, fundus autofluorescence, and optical coherence tomography (OCT) are increasingly being used as complementary tools.5
Only a few reports have been published on the management of recurrent IH in pediatric patients under ATRA treatment. We describe the treatment details of a case with APL and recurrent IH and underline the use of retinal nerve fiber layer (RNFL) thickness as a biomarker.
Case Presentation
A 15-year-old girl presented with a one-month history of left frontal headache associated with blurred vision and relieved by vomiting. Her vision returned to baseline once the pain subsided. She reported recurrent herpes labialis infections for the previous three months, as well as loss of appetite, malaise, and a 7 kg weight loss in the month prior to presentation. The family history was positive for migraine in her aunt and grandmother. Physical and ophthalmological examination findings were unremarkable except for left homonymous hemianopsia. The patient’s body mass index (BMI) was 25 kg/m2 at the 73rd percentile. The complete blood count revealed pancytopenia (white blood cell: 1.2×103/µL, neutrophil count: 0.2 ×103/µL, hemoglobin: 8.8 g/dl, platelet count: 74 ×103/µL). Two atypical cells were detected on the peripheral blood smear. Brain magnetic resonance imaging (MRI) revealed an acute infarction in the territory of the right posterior cerebral artery (PCA) (Supplementary Fig. 1). MR angiography demonstrated that the right distal PCA (P2 segment) was significantly thinner and showed poorer branching compared with the left. Further laboratory investigations for autoimmune and infectious etiologies, including viral serology (herpes simplex virus, varicella zoster virus, human immunodeficiency virus, Epstein-Barr virus, and severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), antinuclear antibodies (ANA), anti-double-stranded DNA (anti-dsDNA), antiphospholipid antibodies, and antineutrophil cytoplasmic antibodies (ANCA), were negative. Bone marrow aspiration revealed a 95% predominance of blast cells and flow cytometric analysis was compatible with APL-M3, confirmed by cytogenetic analysis showing t(15;17). Cerebrospinal fluid (CSF) protein (23 mg/dL), glucose (86 mg/dL), and opening pressure (23 cm H2O) were within normal ranges. CSF cytology revealed no atypical cells. Treatment with ATRA (25 mg/m2/day) and ATO (0.15 mg/kg/day) was started. The course of the treatment and clinical parameters of the patient’s follow-up are shown in Fig. 1.

On day 2 of the second course of ATRA, the patient complained of an itchy, raised maculopapular eruption on the upper limbs that quickly spread to the trunk and lower limbs, and persisted despite the administration of antihistamines and systemic steroids. Skin biopsy was compatible with drug eruption. ATRA and ATO were discontinued. The rash disappeared within 4-5 days. Desensitization was performed prior to restarting the two drugs, and treatment was restarted after 2 weeks.
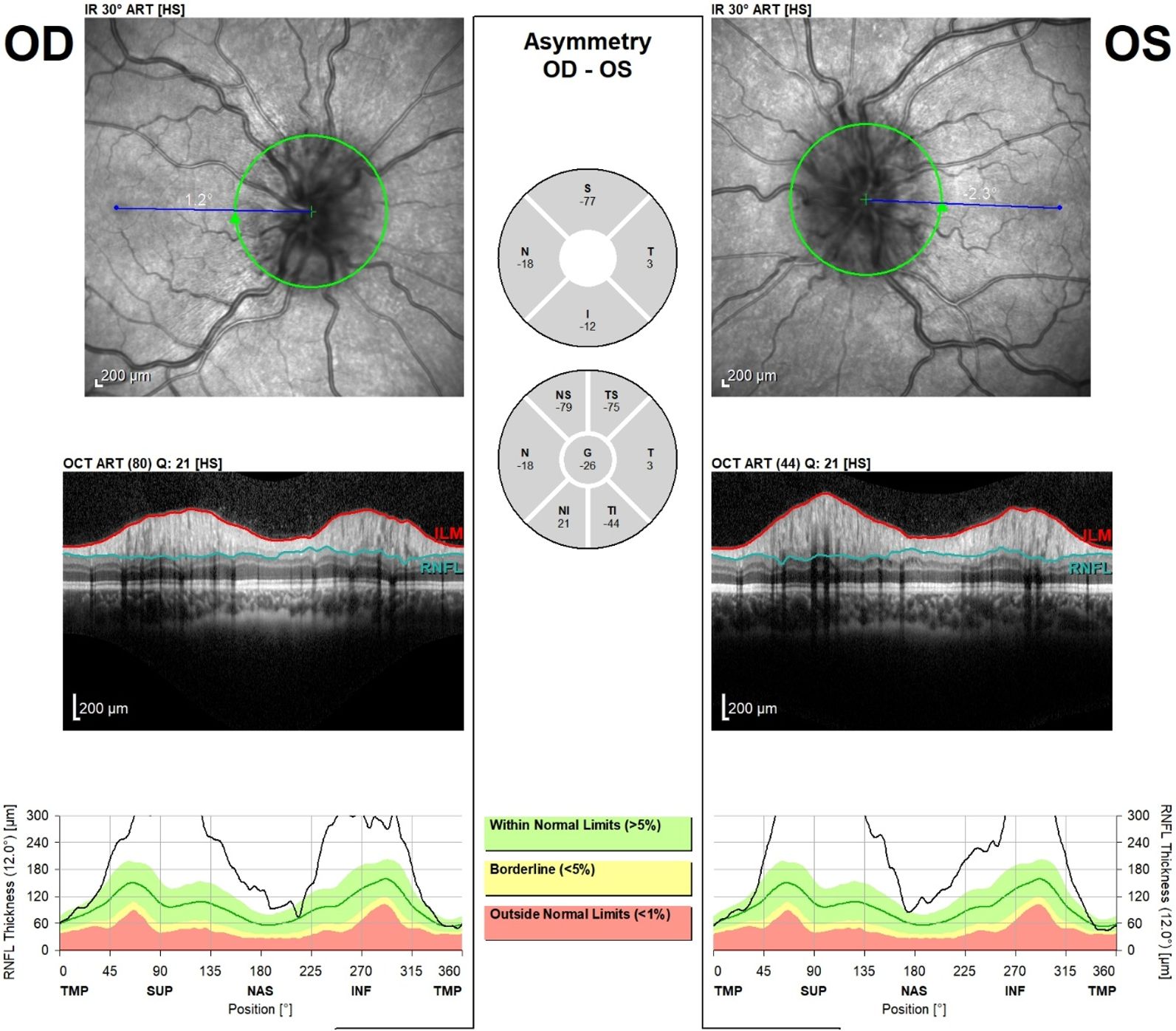
At the end of the third course of ATRA treatment, she presented with headache, vomiting, a new-onset visual field defect in the right eye, and expansion of the previous visual field defect on the left side. Bone marrow aspiration was normal. Ophthalmic examination revealed grade 3 papilledema (Fig. 2) and OCT confirmed thickening of the RNFL (Fig. 3). Brain MRI and MR venography showed no significant findings except for chronic infarction. On LP, the opening pressure was too high to measure, and the closing pressure was 30 cm H2O. CSF protein (23.7 mg/dL) and glucose (65 mg/dL) levels were normal; no atypical cells were observed on cytology. The cumulative ATRA dose was determined as 3,360 mg, based on a daily dose of 25 mg/m² for a body surface area of 1.6 m². The patient developed symptoms of intracranial hypertension at the end of the third course of ATRA intake, which may suggest the impact of cumulative toxicity of the drug on the clinical picture. Acetazolamide (10 mg/kg/day) was started, and ATRA was stopped. The headache regressed in 2 days, while metabolic acidosis that developed on day 6 was treated with oral sodium bicarbonate. Because the right-sided visual field defect did not regress and fundus findings did not improve, a therapeutic LP was performed on the 7th day of treatment, where the CSF opening pressure was again not measurable and the closing pressure was 18 cm H2O. The dose of acetazolamide was increased to 22 mg/kg/day, and a single dose of furosemide (1 mg/kg) was given. The right sided visual field defect regressed after one week. The papilledema regressed to grade 2, and the thickness of the RNFL decreased within one week. The dose of sodium bicarbonate was increased according to the metabolic acidosis (serum HCO3- values). After two weeks, the papilledema regressed to grade 1-2. ATRA was restarted at half-dose and increased to the full dose after one week.

After day 12 of the current admission and before the fourth course of ATRA, bone marrow aspiration and LP were repeated to assess CNS remission and intracranial pressure. The CSF results were normal (pressure 24 cmH2O), and ATRA was restarted at half dose, with a plan to increase to full dose after three days. One month later, the patient complained of worsening headaches and vomiting. Although no papilledema was observed, OCT findings revealed increased RNFL thickness and convolution of retinal blood vessels. Repeated brain MRI and venography were normal. Topiramate (0.5 mg/kg/day) was added to acetazolamide. A week later, grade 1-2 papilledema and increased RNFL thickness were observed. The topiramate dosage was increased. However, the ophthalmologic examination two weeks later revealed grade 2 papilledema. The opening and closing CSF pressures were 32 and 21 cm H₂O, respectively. Topiramate was increased to 1.5 mg/kg/day, ATRA was discontinued, and weekly detailed eye examinations were performed. The RNFL thickness was the first finding to show improvement (in week one), the papilledema regressed by week three, and pallor on the nasal side of the optic discs was observed by week four. ATRA treatment was restarted.
After two months, optic disc pallor was more marked, but RNFL thickness was normal. Acetazolamide was tapered off over five weeks. Topiramate was given for one more month after the last ATRA treatment and discontinued within two months during follow-up.
The patient’s planned 7-month, seven-course chemotherapy was completed without other complications over a total of 11 months. There was no relapse of IH and APL during a 2 year-follow-up.
Informed consent was obtained for publication.
Discussion
Acute promyelocytic leukemia is a unique subtype of acute myeloid leukemia (AML) in which the ATRA/ATO combination has transformed a frequently fatal disease into one with a high cure rate. IH is a known complication of ATRA and was reported to be 18% in a single-center study from our country.1,6 There are few reported cases of recurrent IH after reinitiation of ATRA in the literature.2 Montesinos et al.2 found an incidence of IH of 3.1% in all age groups and recurrence of IH despite discontinuation of ATRA in 28% of cases. APL accounts for 5-10% of pediatric AML cases.1 IH risk has been found to be high in pediatric patients, especially during the first 2-3 weeks of APL induction therapy regimens.7 According to the literature, cessation of ATRA is sufficient to resolve IH in approximately 30% of patients.2 In others, drugs such as acetazolamide or topiramate or therapeutic LP may relieve the signs and symptoms, as in our patient.1 The treatment should be tailored according to the patient’s presentation, but reliable parameters are needed for follow-up. Papilledema can last up to 3 months, and treatments like acetazolamide may require adjustments for up to 6 months in IH.8-10 As in our patient, recurrent LP or add-on treatment may be necessary. With improvement in symptoms, ATRA treatment can be resumed. Previously reported pediatric IH cases and their characteristics, as well as the distribution of IH in APL case series are shown in Table I.
|
¶ The day of ATRA treatment, on which IH developed, #total number of patients with IH, ‡mg per day, *during induction, * *during consolidation ATRA, all-trans retinoic acid; BMT, bone marrow transplant; c, continuation; CR, complete remission; d, discontinuation; IH, intracranial hypertension; i, interruption; LP, lumbar puncture (and high CSF pressure was documented); r, dose reduction; y, years |
||||||||
| Table I. All-Trans retinoic acid induced intracranial hypertension in pediatric acute promyelocytic leukemia: case characteristics and series distribution. | ||||||||
| References |
|
|
|
|
|
|
|
|
| Smith et al.15 |
|
|
|
|
|
|
|
|
| Mahmoud et al.16 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Varadi et al.17 |
|
|
|
|
|
|
|
|
| Visani et al.18 |
|
|
|
|
|
|
|
|
| Decaudin et al.19 |
|
|
|
|
|
|
|
|
| Sano et al.20 |
|
|
|
|
|
|
|
|
| Chen et al.21 |
|
|
|
|
|
|
|
|
| Tallman et al.22 |
|
|
|
|
|
|
|
|
| Schroeter et al.23 |
(Intracranial pressure unknown |
|
|
|
|
|
|
|
| Guirgis et al.24 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Vanier et al.25 |
(a leak in the manometer) |
|
|
|
|
|
|
|
| Naithani et al.26 |
|
|
|
|
|
|
|
|
| Labrador et al.27 |
|
|
|
|
|
|
|
|
| Rasul et al.28 |
|
|
|
|
|
|
|
|
| Abla et al.29 |
|
|
|
|
|
|
|
|
| Coombs et al.30 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Schwartz et al.31 |
|
|
|
|
|
|
|
|
| Shirai et al.32 |
|
|
|
|
|
|
|
|
| Molinaro et al.33 |
|
|
|
|
|
|
|
|
| Our case |
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
(PTC incidence) |
|
|
|
||||
| Warrell et al.34 |
|
|
|
|
|
|||
|
|
||||||||
| Frankel et al.35 |
|
|
|
|
|
|||
| Tallman et al.36 |
|
|
|
|
|
|||
| Bapna et al.37 |
|
|
|
|
|
|||
| Mandelli et al.38 |
|
|
|
|
|
|||
|
|
||||||||
|
|
(PTC incidence) |
|
|
|
||||
| Douer et al.39 |
|
|
|
|
|
|||
| Mann et al.40 |
|
|
|
|
|
|||
| Testi et al.41 |
|
|
|
|
|
|||
| Ortega et al.42 |
|
|
|
|
|
|||
| Montesinos et al.2 |
|
|
|
|
|
|||
| Gregory et al.43 |
|
|
|
|
|
|||
| Imaizumi et al.44 |
|
|
|
|
|
|||
| Jeddi et al.45 |
|
|
|
|
|
|||
| Avvisati et al.46 |
|
|
|
|
|
|||
| Dorantes-Acosta et al.47 |
|
|
|
|
|
|||
| Testi et al.48 |
|
|
|
|
|
|||
| Aksu et al.6 |
|
|
|
|
|
|||
| Kutny et al.49 |
|
|
|
|
|
|||
|
|
||||||||
|
|
(PTC incidence) |
|
|
|
||||
| Strocchio et al.50 |
|
|
|
|
|
|||
| Zhang et al.51 |
|
|
|
|
|
|||
| Spezza et al.52 |
|
|
|
|
|
|||
| Breviglieri et al.53 |
|
|
|
|
|
|||
| Khan et al.54 |
|
|
|
|
|
|||
|
|
|
|||||||
| Kutny et al.55 |
|
|
|
|
|
|||
| Testi et al.56 |
|
|
|
|
|
|||
| Vaid et al.57 |
|
|
|
|
|
|||
| Roy et al.58 |
|
|
|
|
|
|||
| Javed et al.59 |
|
|
|
|
|
|||
| Singh et al.60 |
|
|
|
|
|
|||
| Maldonado et al.61 |
|
|
|
|
|
|||
A recent study11 reported that vitamin A derivatives were responsible for 16.2% of cases of drug-induced IH, which is mostly caused by acne medications. These findings indicate that caution should be exercised with regard to IH when using vitamin A and its derivatives for any purpose.
This case illustrates the challenge faced in managing IH in a malignant disease requiring ATRA treatment. Our patient had multiple problems due to her disease: the presentation of APL with ischemic infarction is very rare.12 In our patient, the cerebrovascular complication of APL resulted in visual field defects observed at the time of diagnosis. Their presence complicated the distinction of visual impairment caused by IH. Although APL is a disease prone to thrombosis, the IH due to ATRA is not the result of venous thrombosis. ATRA increases the production of CSF and alters the lipid structure of the arachnoid villi, resulting in impaired CSF reabsorption.1 On the other hand, IH secondary to intracranial leukemic infiltration has also been reported under ATRA treatment.13 Therefore, differential diagnosis is important for treatment and follow-up.
Monitoring of IH is particularly important in cases with recurrent IH. Ophthalmological examination, a practical and non-invasive method, is essential.5 Imaging findings are not sensitive to IH: as in our patient, MRI may be normal and does not reflect changes in IH immediately.14 Measurement of CSF pressure is accurate but requires an invasive procedure. Therefore, sensitive and reliable biomarkers are needed for the detection of IH. In our patient, relying only on symptoms and papilledema only would not have given the chance of adequate and timely treatment, and complications of IH could have developed. According to our experience, measuring RNFL thickness by OCT provides early and objective information.5 In the future OCT may also be used to measure three-dimensional optic nerve head parameters to distinguish IH from other optic neuropathies.14
In our country, OCT is available in training hospitals and university hospitals.
Conclusion
Children with APL treated with ATRA need close follow-up for IH. OCT is helpful in diagnosis, follow-up, and treatment decisions. IH can be resolved, and vision can be preserved by adjusting ATRA doses and administering appropriate drug treatment for IH within an individualized approach.
Acknowledgements
We would like to thank our patient and her parents for supporting this study. Authors would like to thank Dr. Kader Karlı Oğuz from Hacettepe University Faculty of Medicine, Department of Radiology for neuroimaging studies’.
Ethical approval
Since this is a case study, ethical committee approval has not been obtained. Informed consent has been obtained from the family.
Source of funding
The authors declare the study received no funding.
Conflict of interest
The authors declare that there is no conflict of interest.
References
- Gurnari C, Voso MT, Girardi K, Mastronuzzi A, Strocchio L. Acute Promyelocytic Leukemia in Children: A Model of Precision Medicine and Chemotherapy-Free Therapy. Int J Mol Sci 2021; 22: 642. https://doi.org/10.3390/ijms22020642
- Montesinos P, Vellenga E, Holowiecka A, et al. Incidence, Outcome and Risk Factors of Pseudotumor Cerebri after All-Trans Retinoic Acid and Anthracycline-Based Chemotherapy in Patients with Acute Promyelocytic Leukemia. Blood 2008; 112: 2992. https://doi.org/10.1182/blood.V112.11.2992.2992
- Cheng Y, Zhang L, Wu J, Lu A, Wang B, Liu G. Long-term prognosis of childhood acute promyelocytic leukaemia with arsenic trioxide administration in induction and consolidation chemotherapy phases: a single-centre experience. Eur J Haematol 2013; 91: 483-489. https://doi.org/10.1111/ejh.12194
- Friedman DI, Liu GT, Digre KB. Revised diagnostic criteria for the pseudotumor cerebri syndrome in adults and children. Neurology 2013; 81: 1159-1165. https://doi.org/10.1212/WNL.0b013e3182a55f17
- Bassi ST, Pamu R, Ambika S, et al. Optical coherence tomography in papilledema: A probe into the intracranial pressure correlation. Indian J Ophthalmol 2024; 72: 672-676. https://doi.org/10.4103/IJO.IJO_1648_23
- Aksu T, Fettah A, Bozkaya İO, et al. Acute Promyelocytic Leukemia in Children: A Single Centre Experience from Turkey. Mediterr J Hematol Infect Dis 2018; 10: e2018045. https://doi.org/10.4084/MJHID.2018.045
- Ghiaur A, Doran C, Gaman MA, et al. Acute Promyelocytic Leukemia: Review of Complications Related to All-Trans Retinoic Acid and Arsenic Trioxide Therapy. Cancers (Basel) 2024; 16: 1160. https://doi.org/10.3390/cancers16061160
- Loo KG, Lim SA, Lim IL, Chan DW. Guiding follow-up of paediatric idiopathic intracranial hypertension with optical coherence tomography. BMJ Case Rep 2016; 2016: bcr2015213070. https://doi.org/10.1136/bcr-2015-213070
- Cohen Y, Eidel M, Vidan A, Hadar G, Chassid O. A Spectral-Domain-OCT-Guided One-Year Follow-Up of Newly Diagnosed Pediatric Idiopathic Intracranial Hypertension Patients. Diagnostics (Basel) 2026; 16: 457. https://doi.org/10.3390/diagnostics16030457
- Serin HM, Şimşek E, Kanmaz S, et al. Intracranial Hypertension in Children: Etiological, Clinical Features, Treatment and Prognosis. Türkiye Klinikleri J Pediatr 2018; 27: 89-95. https://doi.org/10.5336/pediatr.2018-61528
- Shaia JK, Rock JR, Singh RP, Talcott KE, Cohen DA. Drug-Induced Intracranial Hypertension: The Adverse Effects of Acne Medications and Topical Retinoids. J Neuroophthalmol 2025; 45: 177-182. https://doi.org/10.1097/WNO.0000000000002236
- MacDougall K, Chukkalore D, Rehan M, Kashi M, Bershadskiy A. Acute promyelocytic leukemia presenting as recurrent venous and arterial thrombotic events: a case report and review of the literature. J Community Hosp Intern Med Perspect 2021; 11: 832-838. https://doi.org/10.1080/20009666.2021.1973657
- Nguyen HS, Haider KM, Ackerman LL. Unusual causes of papilledema: Two illustrative cases. Surg Neurol Int 2013; 4: 60. https://doi.org/10.4103/2152-7806.110686
- Prem Senthil M, Anand S, Chakraborty R, et al. Exploring the utility of retinal optical coherence tomography as a biomarker for idiopathic intracranial hypertension: a systematic review. J Neurol 2024; 271: 4769-4793. https://doi.org/10.1007/s00415-024-12481-3
- Smith MA, Adamson PC, Balis FM, et al. Phase I and pharmacokinetic evaluation of all-trans-retinoic acid in pediatric patients with cancer. J Clin Oncol 1992; 10: 1666-1673. https://doi.org/10.1200/JCO.1992.10.11.1666
- Mahmoud HH, Hurwitz CA, Roberts WM, Santana VM, Ribeiro RC, Krance RA. Tretinoin toxicity in children with acute promyelocytic leukaemia. Lancet 1993; 342: 1394-1395. https://doi.org/10.1016/0140-6736(93)92755-i
- Varadi G, Lossos A, Or R, Kapelushnik J, Nagler A. Successful allogeneic bone marrow transplantation in a patient with ATRA-induced pseudotumor cerebri. Am J Hematol 1995; 50: 147-148. https://doi.org/10.1002/ajh.2830500215
- Visani G, Manfroi S, Tosi P, Martinelli G. All-trans-retinoic acid and pseudotumor cerebri. Leuk Lymphoma 1996; 23: 437-442. https://doi.org/10.3109/10428199609054851
- Decaudin D, Adams D, Naccache P, Castagna L, Munck JN. Maintained all-trans retinoic acid therapy in a patient with pseudotumour cerebri despite aggravated symptoms. Leuk Lymphoma 1997; 27: 373-374. https://doi.org/10.3109/10428199709059694
- Sano F, Tsuji K, Kunika N, et al. Pseudotumor cerebri in a patient with acute promyelocytic leukemia during treatment with all-trans retinoic acid. Intern Med 1998; 37: 546-549. https://doi.org/10.2169/internalmedicine.37.546
- Chen HY, Tsai RK, Huang SM. ATRA-induced pseudotumour cerebri-one case report. Kaohsiung J Med Sci 1998; 14: 58-60.
- Tallman MS, Andersen JW, Schiffer CA, et al. Clinical description of 44 patients with acute promyelocytic leukemia who developed the retinoic acid syndrome. Blood 2000; 95: 90-95.
- Schroeter T, Lanvers C, Herding H, Suttorp M. Pseudotumor cerebri induced by all-trans-retinoic acid in a child treated for acute promyelocytic leukemia. Med Pediatr Oncol 2000; 34: 284-286. https://doi.org/bw3c9w
- Guirgis MF, Lueder GT. Intracranial hypertension secondary to all-trans retinoic acid treatment for leukemia: diagnosis and management. J AAPOS 2003; 7: 432-434. https://doi.org/10.1016/j.jaapos.2003.08.005
- Vanier KL, Mattiussi AJ, Johnston DL. Interaction of all-trans-retinoic acid with fluconazole in acute promyelocytic leukemia. J Pediatr Hematol Oncol 2003; 25: 403-404. https://doi.org/10.1097/00043426-200305000-00010
- Naithani R, Kumar R, Mishra P. Pseudotumor cerebri in a child in early phase of induction therapy for APL with ATRA. Indian J Pediatr 2009; 76: 439-440. https://doi.org/10.1007/s12098-009-0134-x
- Labrador J, Puig N, Ortín A, Gutierrez NC, González-Díaz M. Multiple cranial neuropathy and intracranial hypertension associated with all-trans retinoic acid treatment in a young adult patient with acute promyelocytic leukemia. Int J Hematol 2012; 96: 383-385. https://doi.org/10.1007/s12185-012-1134-6
- Rasul FT, Toma AK, Khan AA, Plant GT, Watkins LD. Pseudotumor cerebri presenting with visual failure in promyelocytic leukemia: a case report. J Med Case Rep 2012; 6: 408. https://doi.org/10.1186/1752-1947-6-408
- Abla O, Ribeiro RC. How I treat children and adolescents with acute promyelocytic leukaemia. Br J Haematol 2014; 164: 24-38. https://doi.org/10.1111/bjh.12584
- Coombs CC, DeAngelis LM, Feusner JH, Rowe JM, Tallman MS. Pseudotumor Cerebri in Acute Promyelocytic Leukemia Patients on Intergroup Protocol 0129: Clinical Description and Recommendations for New Diagnostic Criteria. Clin Lymphoma Myeloma Leuk 2016; 16: 146-151. https://doi.org/10.1016/j.clml.2015.11.018
- Schwartz KR, Hanson JM, Friedmann AM. Pediatric Acute Promyelocytic Leukemia Presenting to the Emergency Department as Refusal to Ambulate. Case Rep Emerg Med 2018; 2018: 5241425. https://doi.org/10.1155/2018/5241425
- Shirai R, Tomizawa D, Okamoto R, Matsumoto K, Miyazaki O. Magnetic Resonance Imaging Findings of All-Trans Retinoic Acid-induced Pseudotumor Cerebri in a Child With Acute Promyelocytic Leukemia. J Pediatr Hematol Oncol 2020; 42: 138-140. https://doi.org/10.1097/MPH.0000000000001610
- Molinaro A, Zanta D, Moleti ML, et al. Challenging Management of Severe Differentiation Syndrome in Pediatric Acute Promyelocytic Leukemia Treated with ATRA/ATO. Mediterr J Hematol Infect Dis 2022; 14: e2022027. https://doi.org/10.4084/MJHID.2022.027
- Warrell RP, Frankel SR, Miller WH, et al. Differentiation therapy of acute promyelocytic leukemia with tretinoin (all-trans-retinoic acid). N Engl J Med 1991; 324: 1385-1393. https://doi.org/10.1056/NEJM199105163242002
- Frankel SR, Eardley A, Heller G, et al. All-trans retinoic acid for acute promyelocytic leukemia. Results of the New York Study. Ann Intern Med 1994; 120: 278-286. https://doi.org/10.7326/0003-4819-120-4-199402150-00004
- Tallman MS, Andersen JW, Schiffer CA, et al. All-trans-retinoic acid in acute promyelocytic leukemia. N Engl J Med 1997; 337: 1021-1028. https://doi.org/10.1056/NEJM199710093371501
- Bapna A, Nair R, Tapan KS, et al. All-trans-retinoic acid (ATRA): pediatric acute promyelocytic leukemia. Pediatr Hematol Oncol 1998; 15: 243-248. https://doi.org/10.3109/08880019809028791
- Mandelli F, Diverio D, Avvisati G, et al. Molecular remission in PML/RAR alpha-positive acute promyelocytic leukemia by combined all-trans retinoic acid and idarubicin (AIDA) therapy. Blood 1997; 90: 1014-1021.
- Douer D, Estey E, Santillana S, et al. Treatment of newly diagnosed and relapsed acute promyelocytic leukemia with intravenous liposomal all-trans retinoic acid. Blood 2001; 97: 73-80. https://doi.org/10.1182/blood.v97.1.73
- Mann G, Reinhardt D, Ritter J, et al. Treatment with all-trans retinoic acid in acute promyelocytic leukemia reduces early deaths in children. Ann Hematol 2001; 80: 417-422. https://doi.org/10.1007/s002770100304
- Testi AM, Biondi A, Lo Coco F, et al. GIMEMA-AIEOPAIDA protocol for the treatment of newly diagnosed acute promyelocytic leukemia (APL) in children. Blood 2005; 106: 447-453. https://doi.org/10.1182/blood-2004-05-1971
- Ortega JJ, Madero L, Martín G, et al. Treatment with all-trans retinoic acid and anthracycline monochemotherapy for children with acute promyelocytic leukemia: a multicenter study by the PETHEMA Group. J Clin Oncol 2005; 23: 7632-7640. https://doi.org/10.1200/JCO.2005.01.3359
- Gregory J, Kim H, Alonzo T, et al. Treatment of children with acute promyelocytic leukemia: results of the first North American Intergroup trial INT0129. Pediatr Blood Cancer 2009; 53: 1005-1010. https://doi.org/10.1002/pbc.22165
- Imaizumi M, Tawa A, Hanada R, et al. Prospective study of a therapeutic regimen with all-trans retinoic acid and anthracyclines in combination of cytarabine in children with acute promyelocytic leukaemia: the Japanese childhood acute myeloid leukaemia cooperative study. Br J Haematol 2011; 152: 89-98. https://doi.org/10.1111/j.1365-2141.2010.08332.x
- Jeddi R, Ghédira H, Menif S, et al. Treatment of acute promyelocytic leukemia with PETHEMA LPA 99 protocol: a Tunisian single center experience. Hematology 2010; 15: 204-209. https://doi.org/10.1179/102453309X12583347114176
- Avvisati G, Lo-Coco F, Paoloni FP, et al. AIDA 0493 protocol for newly diagnosed acute promyelocytic leukemia: very long-term results and role of maintenance. Blood 2011; 117: 4716-4725. https://doi.org/10.1182/blood-2010-08-302950
- Dorantes-Acosta E, Medina-Sanson A, Jaimes-García Y, López-Martínez B. Clinical features and treatment outcomes of pediatric acute promyelocytic leukemia in a Mexican pediatric hospital. Rev Invest Clin 2013; 65: 392-398.
- Testi AM, Pession A, Diverio D, et al. Risk-adapted treatment of acute promyelocytic leukemia: results from the International Consortium for Childhood APL. Blood 2018; 132: 405-412. https://doi.org/10.1182/blood-2018-03-836528
- Kutny MA, Geyer S, Laumann KM, et al. Outcome for pediatric acute promyelocytic leukemia patients at Children’s Oncology Group sites on the Leukemia Intergroup Study CALGB 9710 (Alliance). Pediatr Blood Cancer 2019; 66: e27542. https://doi.org/10.1002/pbc.27542
- Strocchio L, Gurnari C, Santoro N, et al. Arsenic trioxide and all-trans retinoic acid treatment for childhood acute promyelocytic leukaemia. Br J Haematol 2019; 185: 360-363. https://doi.org/10.1111/bjh.15507
- Zhang ZX, Lu AD, Wu J, et al. Retrospective analysis of data from 73 patients with childhood acute promyelocytic leukaemia receiving modified chemotherapy: a single-centre study. J Cancer Res Clin Oncol 2021; 147: 1189-1201. https://doi.org/10.1007/s00432-020-03406-4
- Garcia Spezza E, Brethon B, Petit A, et al. Tolerance to arsenic trioxide combined with all-trans-retinoic acid in children with acute promyelocytic leukaemia in France. Br J Haematol 2020; 188: 170-173. https://doi.org/10.1111/bjh.16364
- Breviglieri CNM, de Almeida MTA, Neto GZ, Teixeira RAP, Odone-Filho V, Cristofani LM. Acute promyelocytic leukemia in childhood and adolescence: treatment results of a modified AIDA protocol at a Brazilian center. Hematol Transfus Cell Ther 2023; 45(Suppl 2): S126-S130. https://doi.org/10.1016/j.htct.2022.09.1276
- Khan ER, Islam A, Jamal CY, et al. Outcome and complications of pediatric acute promyelocytic leukemia in Bangladesh. Pediatr Hematol Oncol 2022; 39: 406-417. https://doi.org/10.1080/08880018.2021.2002486
- Kutny MA, Alonzo TA, Abla O, et al. Assessment of Arsenic Trioxide and All-trans Retinoic Acid for the Treatment of Pediatric Acute Promyelocytic Leukemia: A Report From the Children’s Oncology Group AAML1331 Trial. JAMA Oncol 2022; 8: 79-87. https://doi.org/10.1001/jamaoncol.2021.5206
- Testi AM, Al-Jadiry MF, Ghali HH, et al. Childhood acute promyelocytic leukemia in a pediatric cancer referral center in Baghdad, Iraq. Improved results with ATRA extended consolidation. Leuk Lymphoma 2022; 63: 2940-2947. https://doi.org/10.1080/10428194.2022.2105328
- Vaid T, Aggarwal M, Dass J, et al. Shifting gears to differentiation agents in acute promyelocytic leukemia with resource constraints-a cohort study. Acta Oncol 2022; 61: 1050-1055. https://doi.org/10.1080/0284186X.2022.2109424
- Roy PS, Munikoty V, Trehan A, et al. Early mortality continues to be a barrier to excellent survival in childhood acute promyelocytic leukemia: a retrospective study of 62 patients spanning 17 years. Pediatr Hematol Oncol 2023; 40: 117-130. https://doi.org/10.1080/08880018.2022.2082610
- Javed H, Chudary QU, Iftikhar R, Shahbaz N, Ali M, Hamayun S. Treatment Outcomes Of Patients With Newly Diagnosed Acute Promyelocytic Leukemia; Experience From A Developing Country. J Ayub Med Coll Abbottabad 2022; 34: 791-796. https://doi.org/10.55519/JAMC-04-10127
- Singh C, Yanamandra U, Karunakaran P, et al. Long-term real-world outcomes of patients with acute promyelocytic leukaemia treated with arsenic trioxide and all-trans retinoic acid without chemotherapy-a retrospective, single-centre study. Br J Haematol 2023; 201: 249-255. https://doi.org/10.1111/bjh.18618
- Murillo-Maldonado MA, Galván PG, Ortega IP, Morales FG, Villegas LJ, Acosta ED. Long-term experience in treatment of acute promyelocytic leukemia in Mexican children in a tertiary care hospital. Front Oncol 2023; 13: 1286106. https://doi.org/10.3389/fonc.2023.1286106
Copyright and license
Copyright © 2026 The Author(s). This is an open access article distributed under the Creative Commons Attribution License (CC BY), which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is properly cited.









