
Graphical Abstract
Abstract
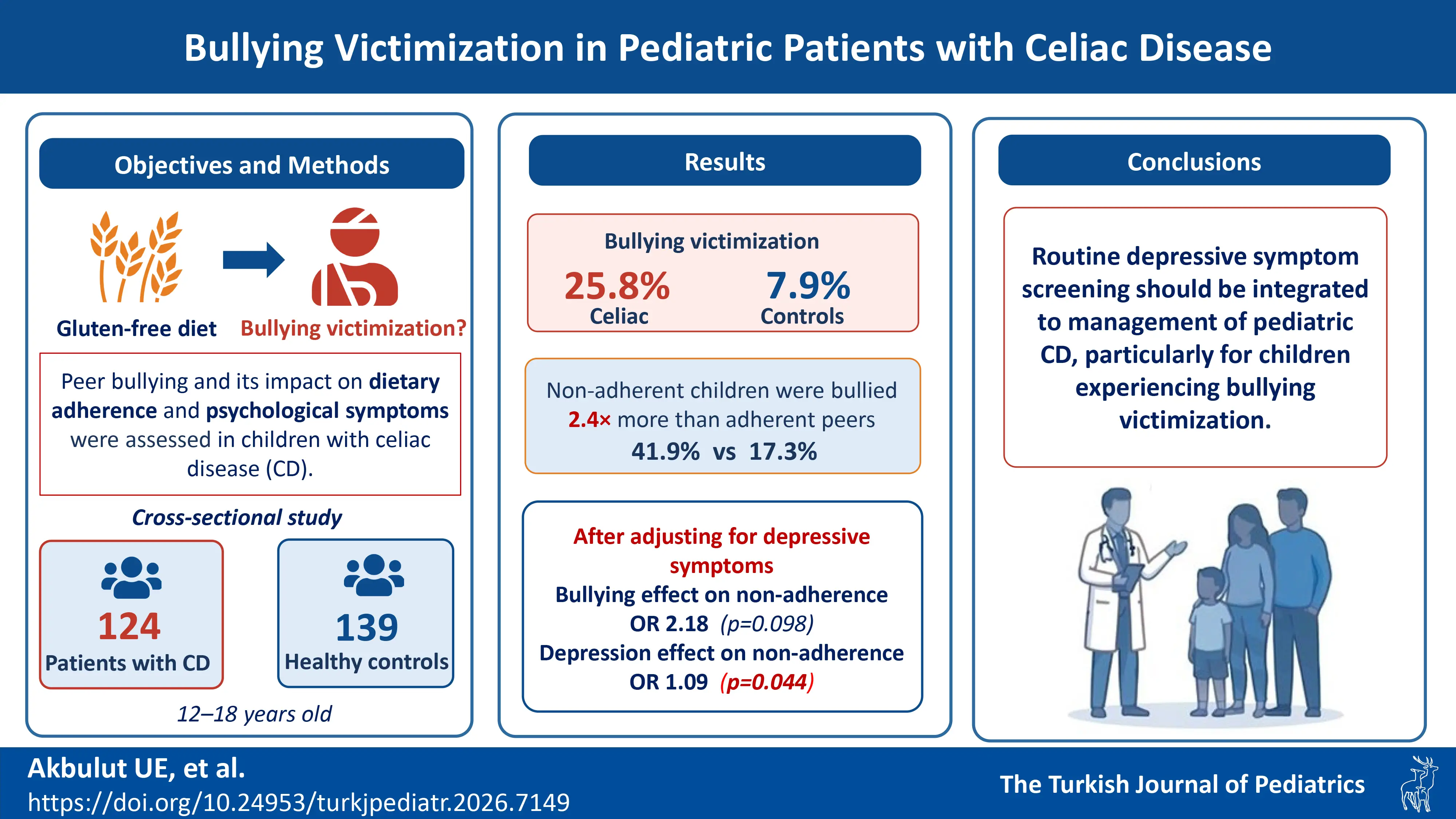
Background. In this study, we aimed to investigate peer bullying and its psychosocial consequences in children with celiac disease. We examined the relationship between adherence to diet and anxiety and depressive symptoms.
Methods. The sample in this cross-sectional study consisted of 124 pediatric celiac patients on a gluten-free diet for one year or more. One hundred thirty-nine healthy children comparable in age and sex were enrolled as the control group. The Revised Olweus Bully Victim Questionnaire (OBVQ) was used to evaluate the peer victimization. The Revised Child Anxiety and Depression Scale and Strengths and Difficulties Questionnaire were used to assess children’s anxiety and depressive symptoms, and emotional and behavioral symptoms, respectively. Hierarchical logistic regression analysis was performed to identify independent predictors of dietary non-adherence.
Results. The proportion of children classified as bullying victims based on the OBVQ was significantly higher in the celiac disease group than in the healthy controls. Children who did not comply with diet therapy experienced significantly higher rates of peer bullying than those who adhered to the diet (p=0.004). However, multivariate analysis indicated that depressive symptoms appeared to account for this relationship - while bullying initially predicted dietary non-adherence (odds ratio [OR]: 3.274, p=0.004), this effect became non-significant when depression was controlled (OR: 2.177, p=0.098), whereas depression remained a significant independent predictor (OR: 1.093, p=0.044). Significant positive correlations were observed between peer bullying and anxiety and depression symptom scores. Peer bullying also exhibited positive correlations with emotional and behavioral symptoms.
Conclusions. The study findings show that children with celiac disease experience higher rates of peer bullying than their healthy peers. More importantly, our results suggest that the association between bullying and dietary adherence may be largely explained by co-occurring depressive symptoms. We therefore recommend that depressive symptom screening and treatment should be integrated into the management of celiac disease in children, particularly for those experiencing peer victimization.
Keywords: victim, psychiatric disorders, depressive symptoms, anxiety symptoms, gluten-free diet
Introduction
Celiac disease (CD) is a chronic, gluten induced enteropathy that occurs in genetically susceptible individuals.1 The prevalence of CD is influenced by genetic and environmental factors, with an estimated occurrence of 0.5-2% in the general population, averaging approximately 1%.2,3 A gluten-free diet (GFD) is so far the only known treatment.4 However, children and adolescents may have problems adhering strictly to this. Children with CD are also at a higher risk of psychological problems, including anxiety and depression.5 These psychological issues can also adversely impact adherence to the GFD.6
Bully victimization refers to intentional, repeated aggressive behaviors directed by more powerful peers against individuals with lower social power.7 Bullying victimization can cause physical and psychological problems in children and can also lead them to engage in more risky behaviors.8,9 Children with chronic illnesses are more vulnerable to bullying victimization, and the victimization they experience during their school years can have lifelong adverse consequences.10,11 Critically, for youth with chronic conditions, peer victimization has been associated with worse disease management and reduced adherence to essential treatment regimens.12 Exposure to bullying victimization among children with CD may impair their adherence to a GFD.
The primary objective of this study was to determine the prevalence of bullying behaviors in children with CD compared with healthy controls. The secondary objectives were i: to investigate whether exposure to peer bullying affects dietary adherence in children with CD, and ii: to explore the psychosocial consequences of being bullied, including emotional and behavioral problems, and anxiety and depressive symptoms.
Materials and Methods
Study design
This study was performed as a cross-sectional analytical investigation with a control group. Children with CD aged 12-18 years participated in the study. Healthy children of similar age and sex distribution comprised the control group. The study protocol was approved by the Antalya Training and Research Hospital Scientific Research Ethics Committee, (Approval Date 09/01/2025, Approval Number 2025-08) prior to commencement. Written and verbal informed consent was obtained from both the participating children and their parents prior to enrollment. The study was conducted in accordance with the Declaration of Helsinki regarding human and animal rights and with local laws and regulations.
Sample size
G Power software version 3.1.9.7 was applied with an alpha of 0.05 (two-sided) and 95% power. The sample size was calculated based on the mean difference between two independent groups (CD and healthy). Means and standard deviation depression values were taken from a previous similar study (CD case 13.9 ± 6.2, healthy control 9.3 ± 4.0).13 Since we used the Strengths and Difficulties Questionnaire (SDQ)14, the expected difference between the two groups was 2, and the minimum required sample size was 100 participants in both groups.
Participants
All patients with a confirmed diagnosis of CD based on the guidelines approved by the European Society for Pediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN)15, and on a GFD for at least one year and who consented to take part were included in the study. Children were excluded if they had an acute illness at the time of recruitment and in the presence of a developmental disability.
Control Group Selection: Children who were comparable in age and sex, and who were examined at the same hospital’s pediatric outpatient clinics due to mild physical symptoms (e.g., common cold and rhinitis) and who had no chronic medical or psychiatric conditions, composed the control group.
Data collection
Sociodemographic data form
This form was designed to collect sociodemographic information about the children and their parents. It included details such as the participants’ age and gender, parental education levels, marital status and ages of the parents’, and the family’s monthly income level. “ family’s monthly income level was categorized as ‘good,’ ‘average,’ or ‘poor’ based on multiples of the national gross minimum wage (MW): ‘poor’ (income < 1 MW), ‘average’ (1–3 MW), and ‘good’ (> 3 MW).
Anthropometric measurements
Measurements of body weight and height were taken when the children were wearing light clothing and were barefoot. Body mass index (BMI) was calculated using the following formula: weight (kg)/ height2 (m2). BMI z-score was calculated according to the standards defined by the World Health Organization.16
The Strengths and Difficulties Questionnaire (SDQ)
The SDQ is a behavioral screening questionnaire developed by Goodman et al. in 1997 to assess parents’ perceptions of both positive (prosocial) and challenging behaviors in children.14 It consists of 25 items grouped into five subscales: (i) conduct problems, (ii) hyperactivity/inattention, (iii) emotional symptoms, (iv) peer relationship problems, and (v) prosocial behavior. Higher scores on the first four subscales indicate behavioral difficulties. The sum of these four subscales yields the “total difficulties score”. The prosocial behavior score reflects positive social behaviors and is interpreted separately as a strength, rather than as a problem area. In addition to the subscale scores, we calculated two composite scores as recommended in the SDQ literature: the internalizing problems score (sum of the emotional problems and peer relationship problems subscales) and the externalizing problems score (sum of the conduct problems and hyperactivity-inattention subscales). The Turkish adaptation by Güvenir et al. demonstrated good reliability, with a Cronbach alpha of 0.73.17
The Revised Child Anxiety and Depression Scale (RCADS)
Developed in 2010 as a screening tool for anxiety disorders and depression in children and adolescents18, the RCADS exists in both child and parent report versions. The present study employed the child self-report form. The scale uses a four-point Likert-type scoring system (0=Never, 1=Sometimes, 2=Often, 3=Always) and consists of 47 items. RCADS consists of six subscales: social phobia, panic disorder, major depressive disorder, separation anxiety, generalized anxiety, and obsessive-compulsive disorder. Eight scores can be calculated upon completion of the scale. There are six individual subscale scores, a total anxiety score (sum of five anxiety subscales), and a total internalizing score (combined anxiety and depression). The validity and reliability study for the Turkish version was conducted by Görmez et al., and confirmatory factor analysis confirmed the original six-factor structure. The internal consistency of the Turkish version of the scale is strong/excellent, with a Cronbach alpha score of 0.95. Cronbach alpha values for the subscales range from 0.75 to 0.86.19 In this study, we employed raw RCADS scores rather than age- and gender-adjusted T-scores to enable straightforward comparisons of mean values between the study groups.
Revised Olweus Bully Victim Questionnaire (OBVQ)
Originally developed by Dan Olweus in 199620, the OBVQ is a 39-item instrument that includes a detailed definition of peer bullying. The questionnaire assesses retrospective recall, with items phrased “In the past few months...” to capture recent experiences. The answers to the questions are defined in detail (e.g., “This hasn’t happened to me/I haven’t bullied others in the past months,” “Only once or twice,” “2 or 3 times a month,” “About once a week,” or “Several times a week”). In order to classify an individual as a bully or victim, these behaviors are expected to occur “2 or 3 times a month or more.” Marking any answer above the cut-off point in questions 4-13 of the questionnaire indicates victim status, while meeting the same condition in questions 24-33 indicates bullying. Adolescents who meet the assessment criteria in both the bully and victim sections of the questionnaire are classified as bully/victim. For the primary analyses in this study, OBVQ responses were used to create a dichotomous variable indicating peer victimization status (victim present vs. absent). The original questionnaire was adapted into Turkish by Sipahi et al., with a Cronbach alpha value of 0.81.21
Celiac serology
Serum anti-tissue transglutaminase IgA (tTG IgA) levels were measured using standardized ELISA kits (Inova Inc., San Diego, CA, USA) according to the manufacturer’s instructions. Briefly, microplates were pre-coated with human tissue transglutaminase antigen. Donor plasma samples were incubated in antigen-coated plates. Unbound antibodies were removed through standardized washing procedures. Next, an enzyme-linked anti-human IgA conjugate was added, chromogenic substrate was added for enzymatic color development, and optical density was measured using an integrated plate reader. tTG IgA levels >20 U/L were considered indicative of non-adherence to GFD in the CD patients and of potential ongoing gluten exposure. For comparative purposes, continuous tTG IgA values are also reported.
Statistical analysis
Statistical evaluations were performed using Statistical Package for the Social Sciences (SPSS) software for Windows version 26.0 (IBM Corp., Armonk, NY, USA). Normality of distribution was evaluated using the Kolmogorov-Smirnov test. In comparisons between the CD and control groups, the independent sample t test was applied for normally distributed data and the Mann-Whitney U test for non-normally distributed data. Categorical data were compared using the chi-square test. Descriptive statistical values including mean and standard deviation were presented for continuous data, and median and interquartile range (IQR) for non-parametric data. In evaluating relationships between the sociodemographic data and scale scores of the celiac and control groups, Pearson’s correlation analysis was used for parametric data, and Spearman’s correlation analysis for non-parametric data. For correlations involving the dichotomous peer victimization variable, point-biserial correlation coefficients are reported. Logistic regression analysis was conducted to evaluate the factors affecting peer bullying.
In addition, we conducted multivariate logistic regression to identify independent predictors of dietary non-adherence. The analysis followed a hierarchical approach with three sequential models: Model 1 examined the crude effect of peer victimization (present/absent) on dietary adherence; Model 2 adjusted for psychological covariates including depression scores (from RCADS) and emotional problems (from SDQ); Model 3 further controlled for demographic variables (age and gender). This model building strategy allowed us to examine whether the effect of bullying on dietary adherence was attenuated by psychological factors. Model fit for each step of the hierarchical logistic regression was assessed using the -2 log likelihood statistic, model chi-square (χ²) with degrees of freedom (df) and p-value, Nagelkerke’s R², and the change in R² (ΔR²) between successive models. The goodness-of-fit for the final model was evaluated using the Hosmer-Lemeshow test, and its overall classification accuracy was reported. The hierarchical (blockwise) entry of variables was based on a conceptual framework regarding their temporal and theoretical relationships. In the first model (Model 1), only peer victimization was entered to examine its unadjusted (crude) association with dietary adherence. In the second model (Model 2), psychological variables (depressive symptoms and emotional problems) were added. This step tested whether the initial association between bullying and adherence could be explained by these potential psychological consequences of victimization. In the final model (Model 3), demographic variables (age and sex) were included to control for potential confounding and to examine whether the observed relationships were independent of these basic characteristics. Sociodemographic characteristics (age, sex, parental education and income) were also compared between diet-adherent and non-adherent celiac patients using independent samples t-test, Mann-Whitney U test, or chi-square test, as appropriate. A p value of < 0.05 was considered statistically significant.
Results
A total of 290 individuals were assessed for eligibility. Of these, 8 were excluded due to acute disease, 4 had incomplete clinical data, and 15 declined to participate. The remaining 263 children were included in the final analysis, comprising 124 patients with celiac disease and 139 healthy controls. All participants were recruited from the Antalya Education and Research Hospital Pediatric Gastroenterology Department between 01 January and 30 June, 2025.
Sociodemographic characteristics
The participants’ baseline characteristics are shown in Table I. The median age of the 263 children in the study was 13.5 years (IQR: 8-17), and 68.4% were girls. There was no significant difference between the two groups in terms of age, gender, education level, maternal age, paternal age, maternal and paternal education levels, or family income status (p>0.05).
|
Data are presented as mean ± standard deviation, median (interquartile range), or number (percentage). Superscript letters indicate the statistical test used to obtain the p-value: a independent samples t-test; b Mann-Whitney U test; c chi-square test. All p-values are two-sided. BMI: body mass index, IQR: interquartile range, SD: standard deviation. |
|||
| Table I. The participants’ sociodemographic characteristics. | |||
|
|
|
|
|
| Age (yr), mean ± SD |
|
|
|
| Sex, n (%) |
|
||
| Male |
|
|
|
| Female |
|
|
|
| BMI z-score, mean ± SD |
|
|
|
| Maternal age, median (IQR) |
|
|
|
| Paternal age, mean ± SD |
|
|
|
| Maternal education, n (%) |
|
||
| Illiterate |
|
|
|
| Elementary education |
|
|
|
| High school |
|
|
|
| Higher or beyond |
|
|
|
| Paternal education, n (%) | |||
| Illiterate |
|
|
|
| Elementary education |
|
|
|
| High school |
|
|
|
| Higher or beyond |
|
|
|
| Marital status, n (%) | |||
| Married |
|
|
|
| Divorced |
|
|
|
| Household income, n (%) | |||
| Good |
|
|
|
| Average |
|
|
|
| Poor |
|
|
|
| Residential area, n (%) | |||
| Rural |
|
|
|
| Urban |
|
|
|
A comparison of scales between the CD and control groups
Assessment of peer victimization using the OBVQ (Table II), revealed that 25.8% of children with CD met the criteria for victim status, while 1.6% engaged in bullying behavior. In the control group, these rates were 7.9% and 2.9%, respectively. Children with CD experienced bullying significantly more frequently than the healthy controls (p=0.013, odds ratio [OR]: 6.78). Table III compares the SDQ and RCADS scores between the CD and control groups. There was no difference between the groups in terms of anxiety and depressive symptom scores. The total difficulties scores in the SDQ were also similar between the groups. However, among the SDQ subscales, emotional problems were significantly higher in the CD patients (3.76±2.74 vs. 3.09±2.71, p=0.047).
|
Note: Data are presented as number (percentage). OR, odds ratio; CI, confidence interval. p-values were calculated using the chi-square test. The reference category for the upper panel is the absence of celiac disease; for the lower panel, it is dietary adherence. CI: Confidence Interval; OBVQ: Revised Olweus Bully Victim Questionnaire; OR: Odds ratio. |
||||
| Table II. Comparison of peer victimization status based on the Revised Olweus Bully Victim Questionnaire between celiac patients and healthy controls, and according to dietary adherence within the celiac group. | ||||
| OBVQ Status |
|
|
|
|
| Victim only |
|
|
|
|
| Bully only |
|
|
|
|
| Bully + Victim |
|
|
|
|
| OBVQ Status |
|
|
|
|
| Victim only |
|
|
|
|
| Bully only |
|
|
|
|
| Bully + Victim |
|
|
|
|
|
Data are presented as mean ± SD and median (IQR). All comparisons between the celiac disease patients and the control group were performed using the Mann-Whitney U test. *Statistically significant IQR: interquartile range; RCADS: Revised Child Anxiety and Depression Scale; SD: standard deviation; SDQ: Strengths and Difficulties Questionnaire. |
||||
| Table III. A comparison of Strengths and Difficulties Questionnaire, and Revised Child Anxiety and Depression Scale between the celiac disease patients and control group. | ||||
|
|
|
|
|
|
| SDQ | ||||
| Emotional problems |
|
|
|
|
| Conduct problems |
|
|
|
|
| Hyperactivity-inattention |
|
|
|
|
| Peer relationship problems |
|
|
|
|
| Pro-social behavior |
|
|
|
|
| SDQ Internalizing score |
|
|
|
|
| SDQ Externalizing score |
|
|
|
|
| Total difficulties score |
|
|
|
|
| RCADS | ||||
| Separation anxiety disorder |
|
|
|
|
| Generalized anxiety disorder |
|
|
|
|
| Panic disorder |
|
|
|
|
| Social phobia |
|
|
|
|
| Obsessive−compulsive disorder |
|
|
|
|
| Major depressive disorder |
|
|
|
|
| Total anxiety score |
|
|
|
|
| Total score |
|
|
|
|
A comparison of scales according to dietary adherence
When the CD patients were divided into two subgroups based on GFD adherence, non-adherent children experienced significantly higher rates of peer bullying than those who adhered to the diet (41.9% vs 17.3%, respectively; Table II). SDQ subscale analysis revealed that non-adherent children exhibited more severe emotional problems, conduct issues, hyperactivity-inattention difficulties, and peer relationship problems than their diet- adherence counterparts. Notably, children with poor dietary adherence exhibited significantly elevated anxiety and depressive symptom scores on the RCADS compared to the control group. The most pronounced difference emerged in major depressive disorder scores (non-adherent group 10.95±6.53 vs 6.59±5.16, p<0.001), highlighting the substantial psychological burden associated with GFD non-adherence (Table IV). In addition, sociodemographic characteristics of diet-adherent and non-adherent patients are presented in Supplementary Table S1. The groups did not differ significantly in terms of patient age, sex, or parental age (all p>0.05). However, non-adherent patients had significantly lower levels of maternal and paternal education, lower household income, and were more likely to have parents who were divorced (all p <0.05). As expected, non-adherent patients had significantly higher mean tTG IgA levels compared to adherent patients (100.25 ± 68.10 U/L vs. 8.88 ± 5.90 U/L, p<0.001).
|
Notes: Data are presented as mean ± SD and median (IQR). Superscript letters indicate the statistical test used to obtain the p-value: a independent samples t-test; b Mann-Whitney U test. *Statistically significant BMI, Body mass index; IQR, interquartile range; RCADS, Revised Child Anxiety and Depression Scale; SD, standard deviation; SDQ, Strengths and Difficulties Questionnaire; tTG IgA: anti-tissue transglutaminase immunoglobulin A. |
||||
| Table IV. A comparison of Strengths and Difficulties Questionnaire, and Revised Child Anxiety and Depression Scale, according to dietary adherence in the celiac disease patients. | ||||
|
|
|
|
|
|
| SDQ | ||||
| Emotional problems |
|
|
|
|
| Conduct problems |
|
|
|
|
| Hyperactivity-inattention |
|
|
|
|
| Peer relationship problems |
|
|
|
|
| Pro-social behavior |
|
|
|
|
| SDQ internalizing score |
|
|
|
|
| SDQ externalizing score |
|
|
|
|
| Total difficulties score |
|
|
|
|
| RCADS | ||||
| Separation anxiety disorder |
|
|
|
|
| Generalized anxiety disorder |
|
|
|
|
| Panic disorder |
|
|
|
|
| Social phobia |
|
|
|
|
| Obsessive−compulsive disorder |
|
|
|
|
| Major depressive disorder |
|
|
|
|
| Total anxiety score |
|
|
|
|
| Total score |
|
|
|
|
| tTG IgA level (U/L) |
|
|
|
|
| BMI z-score |
|
|
|
|
Correlations between scale scores for the CD and control groups
The relationships between peer victimization status (a dichotomous variable: present/absent) and the scale scores were analyzed using point-biserial correlation, with results detailed in Table V. In both groups, significant positive correlations were observed between victimization status and the total RCADS score and its subscales, as well as with all SDQ subscales except prosocial behavior, indicating that bullying exposure was consistently associated with greater emotional and behavioral difficulties.
|
This table presents the primary analysis of associations between peer victimization status (a dichotomous variable) and psychological symptom scores. Correlation coefficients (r) for the relationships between peer victimization (a dichotomous variable: present/absent) and continuous scale scores are point-biserial correlations. All p-values are two-sided. *Statistically significant BMI, Body mass index; OBVQ, Revised Olweus Bully Victim Questionnaire; RCADS, Revised Child Anxiety and Depression Scale; SDQ, Strengths and Difficulties Questionnaire. |
||||
| Table V. Point-biserial correlations between OBVQ victimization status (present/absent) and psychological symptom scores (SDQ, RCADS) and BMI z-score in children with celiac disease and healthy controls. | ||||
|
|
|
|||
|
|
|
|
|
|
| SDQ | ||||
| Emotional problems |
|
|
|
|
| Conduct problems |
|
|
|
|
| Hyperactivity- inattention |
|
|
|
|
| Peer relationship problems |
|
|
|
|
| Pro-social behavior |
|
|
|
|
| Total difficulties score |
|
|
|
|
| RCADS | ||||
| Separation anxiety disorder |
|
|
|
|
| Generalized anxiety disorder |
|
|
|
|
| Panic disorder |
|
|
|
|
| Social phobia |
|
|
|
|
| Obsessive−compulsive disorder |
|
|
|
|
| Major depressive disorder |
|
|
|
|
| Total anxiety score |
|
|
|
|
| Total score |
|
|
|
|
| BMI z-score |
|
|
|
|
Multivariate logistic regression analysis for dietary non-adherence
The hierarchical logistic regression analysis revealed significant findings regarding predictors of dietary non-adherence (Table VI). In the unadjusted Model 1, peer bullying showed a strong and significant association with dietary non-adherence (OR: 3.274, 95% confidence interval [CI]: 1.466–7.309, p=0.004), indicating that bullied children had approximately 3.3 times higher odds of being non-adherent to the GFD compared to non-bullied children. When psychological factors (depressive symptoms and emotional problems) were added in Model 2, the magnitude and significance of the association for peer bullying were substantially attenuated (OR: 2.035, 95% CI: 0.827–5.005, p=0.122), while depressive symptoms emerged as a significant predictor (OR: 1.085, 95% CI: 1.000–1.178, p=0.045). In the adjusted Model 3, which also included demographic variables (age and gender), depressive symptoms remained a significant independent predictor of dietary non-adherence (OR: 1.093, 95% CI: 1.002–1.192, p=0.044). In this final model, peer bullying (OR: 2.177, 95% CI: 0.867–5.467, p=0.098), emotional problems, age, and gender were not significantly associated with dietary adherence.
|
Reference category for the dependent variable: Dietary compliance. OR > 1 indicates a higher likelihood of dietary non-adherence for the specified category (e.g., presence of peer victimization) compared to the reference category. Model 1: Crude effect of peer victimization. Model 2: Adjusted for psychological factors (depressive symptoms and emotional problems). Model 3: Fully adjusted model (demographic factors). Model Fit Indices: Model 1: χ²(1) = 8.52, p = 0.004; Nagelkerke R² = 0.092; ΔR² (from null) = 0.092. Model 2: χ²(3) = 21.40, p < 0.001; Nagelkerke R² = 0.219; ΔR² (from Model 1) = 0.127. Model 3: χ²(5) = 22.87, p < 0.001; Nagelkerke R² = 0.232; ΔR² (from Model 2) = 0.013; Hosmer-Lemeshow χ²(8) = 5.14, p = 0.742; Classification Accuracy = 72.6%. *p < 0.01, **p < 0.05 BMI, Body mass index; CI, Confidence Interval; OBVQ, Revised Olweus Bully Victim Questionnaire; OR, Odds ratio; RCADS, Revised Child Anxiety and Depression Scale; SDQ, Strengths and Difficulties Questionnaire. |
||||
| Table VI. Hierarchical logistic regression analysis of factors associated with dietary non-adherence in children with celiac disease. | ||||
| Model and Fit Indices | Variable |
(95% CI) |
(95% CI) |
(95% CI) |
| Model 1 | OBVQ victim status (Present vs. Absent) |
|
|
|
| -2 Log likelihood=151.548 | ||||
| Nagelkerke R²=0.092 | ||||
| Model 2 | OBVQ victim status (Present vs. Absent) |
|
|
|
| -2 Log likelihood=138.671 | RCADS, Major depressive disorder |
|
|
|
| Nagelkerke R²=0.219 | SDQ, Emotional problems |
|
|
|
| Model 3 | OBVQ victim status (Present vs. Absent) |
|
|
|
| -2 Log likelihood=137.200 | RCADS, Major depressive disorder |
|
|
|
| Nagelkerke R2 =0.232 | SDQ, Emotional problems |
|
|
|
| Gender (Female vs. Male) |
|
|
|
|
| BMI z-score |
|
|
|
|
| Age |
|
|
|
|
Potential role of anthropometric measures
To address the potential confounding role of growth parameters, we examined the relationship between BMI z-scores and peer victimization. In the entire sample, children who were victims of bullying had significantly lower BMI z-scores compared to non-victims (victims: -0.34 ± 0.96 vs. non-victims: 0.11 ± 0.69; t=3.534, p<0.001). This was consistent with a significant, weak negative correlation between BMI z-score and victimization status (Spearman’s rho = -0.176, p=0.007). Within the celiac disease group, a similar pattern was observed: victims tended to have lower BMI z-scores than non-victims, although this difference was of borderline statistical significance (victims: -0.46 ± 1.14 vs. non-victims: 0.01 ± 0.79; t=2.129, p=0.036). To assess whether growth parameters confounded the main relationship of interest, we examined the association between peer victimization status and BMI z-score (Table V). Furthermore, we incorporated BMI z-score as an additional covariate in Model 3 of our hierarchical regression analysis (Table VI). BMI z-score was not a significant predictor of dietary non-adherence in the final model (OR=1.304, p=0.449), and its inclusion did not alter the fundamental pattern of results.
Discussion
This study represents the first investigation of peer bullying among children with CD. The findings demonstrate that children with the disease experience significantly higher rates of peer victimization compared to their healthy peers. Furthermore, within the CD group, children with poorer adherence to the GFD were more frequently subjected to bullying and exhibited higher levels of anxiety and depressive symptoms.
However, our hierarchical logistic regression analysis revealed a more nuanced relationship: while peer bullying initially showed a strong association with dietary non-adherence, this association was substantially attenuated and lost statistical significance when depressive symptoms were included in the model. This finding suggests that depressive symptoms are a key factor in understanding the link between bullying and dietary non-adherence in this population. The attenuation of the bullying effect when controlling for depressive symptoms is consistent with the possibility that the link between bullying and non-adherence is strongly influenced by, or occurs alongside, depressive symptoms. These results may indicate that peer bullying substantially exacerbates depressive symptoms and adversely affects emotional-behavioral functioning in this population.
Existing research into children with chronic illnesses has consistently demonstrated increased vulnerability to peer bullying compared to healthy peers.10,11 CD is a chronic condition requiring strict lifelong adherence to GFD as the only known treatment. This study confirms that children with CD experience significantly higher rates of peer bullying than their healthy peers. This finding is of particular clinical relevance due to the well-documented challenges of maintaining dietary adherence during childhood.22,23 The high prevalence of peer victimization in this population may further compromise GFD adherence, creating a detrimental cycle. Indeed, the results of this study specifically showed that patients with poorer dietary adherence experienced significantly greater exposure to peer bullying, though our multivariate analyses indicate that this relationship is closely associated with, and may be influenced by, psychological factors, rather than representing a simple direct link. Furthermore, children who were victims of bullying had significantly lower BMI z-scores. This suggests that growth delay or lower body weight—common features in poorly controlled celiac disease—may contribute to the increased vulnerability to peer victimization, potentially by making children appear more physically distinct or vulnerable. However, when the BMI z-score was included as a covariate in our multivariate model predicting dietary non-adherence, it was not a significant independent predictor. This critical finding indicates that while physical factors like lower BMI may be associated with a higher risk of being bullied, they do not directly explain the link between victimization and poor dietary management.
The literature describes various psychiatric disorders associated with CD. While some adult studies report depression as a common comorbidity in such patients24, others have observed no difference compared to the general population.25 Although not as widely studied as in adults, a large cohort study demonstrated a 1.4-fold increased risk of psychiatric disorders in pediatric CD patients versus the general population.26 Similarly, a study evaluating 73 children (42 with CD) reported that psychiatric difficulties were more common in children with CD. However, Esenyel et al.’s smaller study observed no difference in psychiatric symptoms between CD children and controls.27 Another small-sample study showed no significant difference in depression scores between CD patients and healthy children, though better dietary adherence was correlated with significantly lower depressive symptom scores.28 The present study determined no differences in anxiety, depressive symptoms, or psychiatric difficulties between the CD patients and controls overall. However, patients with poor dietary adherence exhibited markedly worse psychiatric outcomes than adherent patients. Notably, depressive symptoms emerged as the most consistent predictor of dietary non-adherence in our multivariate models, remaining significant even after controlling for bullying and other psychological factors. Research has suggested that the effects of inflammation and autoimmunity on the gut-brain axis may contribute to anxiety and other psychiatric disorders. Gluten-derived peptides may affect brain function.29,30 Furthermore, the gut microbiota is known to influence mood and behavior, and changes in the gut microbiota of patients with CD may lead to psychiatric problems such as anxiety and depressive symptoms.31
Furthermore, our supplementary analyses revealed that children with dietary non-adherence came from families with significantly lower socioeconomic status, including lower parental education and income, and were more likely to have parents who were divorced. This finding aligns with broader literature on chronic illness management, where socioeconomic disadvantage is a known barrier to treatment adherence.12 Lower family resources may limit access to gluten-free alternatives, reduce parental capacity to monitor diet, and increase general household stress, all of which could contribute to both non-adherence and vulnerability to psychosocial difficulties such as depressive symptoms. Importantly, in our hierarchical regression models, the association between peer bullying victimization and dietary non-adherence was attenuated when psychological symptoms were controlled for. This suggests that the link between bullying and non-adherence is not merely a reflection of these underlying socioeconomic disparities, but rather operates through the psychological sequelae of victimization.
Our findings have important clinical implications. The observation that the bullying-adherence association was attenuated by depressive symptoms suggests that interventions targeting depressive symptoms may be particularly effective in improving dietary adherence among bullied children with CD. Routine depressive symptom screening should be considered in the follow-up of pediatric celiac patients, especially those reporting peer victimization. While anti-bullying interventions remain important, our results indicate they should be complemented with psychological support addressing the depressive symptoms that are strongly associated with poor dietary adherence.
Another important finding of this study involves the significant mental health impacts of bullying victimization, with bullied students exhibiting markedly higher levels of anxiety and depressive symptoms, stress, behavioral problems, peer relationship difficulties, and overall psychological distress compared to non-victimized peers. These results corroborate previous extensive research documenting strong associations between bullying victimization and mental health problems including depression, anxiety, and general health impairments.8,9,32 Exposure to bullying may lead to unmanaged stress that triggers depressive symptoms and anger, while longitudinal studies confirm bullied children’s heightened long-term vulnerability to anxiety and depressive disorders.10,11 The particularly high prevalence of peer bullying among patients with CD underscores the critical need for closer mental health monitoring in this population compared to healthy children, along with prioritized anti-bullying interventions to reduce anxiety and depressive symptoms and mitigate stress responses in these patients.
This study has several notable strengths, including the inclusion of a large pediatric CD population across a broad age range and the use of validated instruments to assess peer bullying, anxiety-depressive symptoms, and emotional-behavioral problems. Additionally, the use of hierarchical logistic regression allowed us to examine the complex relationships between bullying, psychological factors, and dietary adherence. However, the limitations of the study can be listed as follows. First, the cross-sectional design may limit our ability to establish direct causal relationships between variables. Specifically, while our findings suggest depressive symptoms are a key factor in the bullying-diet adherence relationship, longitudinal studies are needed to confirm this temporal sequence. Second, the study was conducted at a tertiary referral center specializing in CD, which may have introduced selection bias. Third, peer bullying, anxiety and depressive symptom scores were based on self-reports, potentially introducing bias due to participants’ subjective perceptions. In order to partially address this limitation, we supplemented child-reported data with parent-reported assessments using the SDQ to evaluate family attitudes toward children with CD. Fourth, the assessment of psychiatric symptoms relied solely on rating scales (RCADS, SDQ) without confirmation through structured clinical interviews. Therefore, our findings pertain to the level of symptomatology and not to clinically verified diagnoses of depressive or anxiety disorders. Fifth, the RCADS scores are presented as raw scores rather than age- and gender-adjusted T scores. Although this approach is suitable for the group comparisons central to our analysis, it may limit the direct clinical interpretability of individual scores relative to normative data.
Conclusion
This study demonstrates a significant association between CD and peer bullying in childhood. Patients with poor adherence to GFD were more frequently exposed to bullying than their diet-adherent counterparts. More importantly, our multivariate analyses suggest that the impact of bullying on dietary adherence is closely linked to, and may be substantially influenced by, depressive symptoms rather than directly. Furthermore, exposure to bullying had substantial adverse effects on mental health. As the first research to evaluate the relationship between bullying victimization and CD, the findings of this study underscore the critical need for psychosocial screening and assessment in this population. The results also highlight the need for greater awareness of how peer bullying may impact GFD adherence in children with CD. Based on our findings, we recommend that depressive symptom screening become a routine component of CD management, particularly for children experiencing peer victimization. Further research is now needed to validate these findings and elucidate the underlying social and psychological mechanisms linking CD and bullying experiences.
Ethical approval
The study was approved by Antalya Training and Research Hospital Scientific Research Ethics Committee (Approval Date 09/01/2025, Approval Number 2025-08). Written informed consent was provided by each participant. All study procedures were performed in accordance with the Declaration of Helsinki.
Source of funding
The authors declare the study received no funding.
Conflict of interest
The authors declare that there is no conflict of interest.
References
- Wall E, Semrad CE. Celiac disease, gluten sensitivity, and diet management. Curr Gastroenterol Rep 2024; 26: 191-199. https://doi.org/10.1007/s11894-024-00931-x
- Catassi C, Verdu EF, Bai JC, Lionetti E. Coeliac disease. Lancet 2022; 399: 2413-2426. https://doi.org/10.1016/S0140-6736(22)00794-2
- Lebwohl B, Rubio-Tapia A. Epidemiology, presentation, and diagnosis of celiac disease. Gastroenterology 2021; 160: 63-75. https://doi.org/10.1053/j.gastro.2020.06.098
- Mearin ML, Agardh D, Antunes H, et al. ESPGHAN position paper on management and follow-up of children and adolescents with celiac disease. J Pediatr Gastroenterol Nutr 2022; 75: 369-386. https://doi.org/10.1097/MPG.0000000000003540
- Germone M, Phu T, Slosky C, et al. Anxiety and depression in pediatric patients with celiac disease: a large cross-sectional study. J Pediatr Gastroenterol Nutr 2022; 75: 181-185. https://doi.org/10.1097/MPG.0000000000003497
- Coburn S, Rose M, Sady M, et al. Mental health disorders and psychosocial distress in pediatric celiac disease. J Pediatr Gastroenterol Nutr 2020; 70: 608-614. https://doi.org/10.1097/MPG.0000000000002605
- Li X, Ng TK, Lee TH, Li CN. Peer victimization among Chinese adolescents: a longitudinal validation study. Psychol Assess 2024; 36: 53-65. https://doi.org/10.1037/pas0001289
- Christina S, Magson NR, Kakar V, Rapee RM. The bidirectional relationships between peer victimization and internalizing problems in school-aged children: an updated systematic review and meta-analysis. Clin Psychol Rev 2021; 85: 101979. https://doi.org/10.1016/j.cpr.2021.101979
- Schacter HL. Effects of peer victimization on child and adolescent physical health. Pediatrics 2021; 147: e2020003434. https://doi.org/10.1542/peds.2020-003434
- Sentenac M, Arnaud C, Gavin A, Molcho M, Gabhainn SN, Godeau E. Peer victimization among school-aged children with chronic conditions. Epidemiol Rev 2012; 34: 120-128. https://doi.org/10.1093/epirev/mxr024
- Kretschmer T, van der Ploeg R, Kaufman T. Peer victimization in early adolescence and maladjustment in adulthood. Eur Child Adolesc Psychiatry 2025; 34: 1011-1024. https://doi.org/10.1007/s00787-024-02532-5
- Cheung T, McDonald C, Setty M, Tsai P, Wadhwani SI. Social adversities associate with worse disease control in pediatric celiac disease. J Pediatr 2025; 276: 114305. https://doi.org/10.1016/j.jpeds.2024.114305
- Ayyıldız D, Demirtaş Z, Kınacı E. Psychiatric difficulties in children with celiac disease and the relationship between adherence to treatment and parental attitudes. Turk J Gastroenterol 2024; 35: 743-749. https://doi.org/10.5152/tjg.2024.23493
- Goodman R. The strengths and difficulties questionnaire: a research note. J Child Psychol Psychiatry 1997; 38: 581-586. https://doi.org/10.1111/j.1469-7610.1997.tb01545.x
- Husby S, Koletzko S, Korponay-Szabó I, et al. European society paediatric gastroenterology, hepatology and nutrition guidelines for diagnosing coeliac disease 2020. J Pediatr Gastroenterol Nutr 2020; 70: 141-156. https://doi.org/10.1097/MPG.0000000000002497
- World Health Organization. Growth reference data for 5-19 years 2007. Available at: http://www.who.int/growthref/who2007_bmi_for_age/en/ (Accessed on Dec 24, 2025).
- Güvenir T, Özbek A, Baykara B, Arkar H, Şentürk B, İncekaş S. Psychometric properties of the Turkish version of the Strengths and Difficulties Questionnaire (SDQ). Turkish Journal of Child and Adolescent Mental Health, 2008; 15: 65-74.
- Chorpita BF, Yim L, Moffitt C, Umemoto LA, Francis SE. Assessment of symptoms of DSM-IV anxiety and depression in children: a revised child anxiety and depression scale. Behav Res Ther 2000; 38: 835-855. https://doi.org/10.1016/s0005-7967(99)00130-8
- Gormez V, Kilincaslan A, Ebesutani C, et al. Psychometric properties of the parent version of the revised child anxiety and depression scale in a clinical sample of Turkish children and adolescents. Child Psychiatry Hum Dev 2017; 48: 922-933. https://doi.org/10.1007/s10578-017-0716-1
- Olweus D. Bully/victim problems in school. Prospects 1996; 26: 331-359. https://doi.org/10.1007/BF02195509
- Sipahi HT, Karababa AA. Olweus öğrenciler için akran zorbalığı anketinin Türkçeye ve Türkiye’ye uyarlanması ve geçerlilik, güvenirlik analizi. Ege Tıp Dergisi 2018; 57: 222-227. https://doi.org/10.19161/etd.417268
- Taşdelen Baş M, Çavuşoğlu H. Evaluation of daily lives of children and adolescents with celiac disease and nursing approaches. Gastroenterol Nurs 2020; 43: 202-213. https://doi.org/10.1097/SGA.0000000000000509
- Meyer S, Rosenblum S. Examining core self-management skills among adolescents with celiac disease. J Health Psychol 2021; 26: 2592-2602. https://doi.org/10.1177/1359105320922304
- Smith DF, Gerdes LU. Meta-analysis on anxiety and depression in adult celiac disease. Acta Psychiatr Scand 2012; 125: 189-193. https://doi.org/10.1111/j.1600-0447.2011.01795.x
- Häuser W, Janke KH, Klump B, Gregor M, Hinz A. Anxiety and depression in adult patients with celiac disease on a gluten-free diet. World J Gastroenterol 2010; 16: 2780-2787. https://doi.org/10.3748/wjg.v16.i22.2780
- Butwicka A, Lichtenstein P, Frisén L, Almqvist C, Larsson H, Ludvigsson JF. celiac disease ıs associated with childhood psychiatric disorders: a population-based study. J Pediatr 2017; 184: 87-93. https://doi.org/10.1016/j.jpeds.2017.01.043
- Esenyel S, Unal F, Vural P. Depression and anxiety in child and adolescents with follow-up celiac disease and in their families. Turk J Gastroenterol 2014; 25: 381-385. https://doi.org/10.5152/tjg.2014.4831
- Simsek S, Baysoy G, Gencoglan S, Uluca U. Effects of gluten-free diet on quality of life and depression in children with celiac disease. J Pediatr Gastroenterol Nutr 2015; 61: 303-306. https://doi.org/10.1097/MPG.0000000000000799
- Parisi P. The relationship between mucosal damage in celiac disease and the risk of neurological and psychiatric conditions is much more complex than previously thought. Eur J Neurol 2018; 25: 797-798. https://doi.org/10.1111/ene.13614
- Sacchetti L, Nardelli C. Gut microbiome investigation in celiac disease: from methods to its pathogenetic role. Clin Chem Lab Med 2020; 58: 340-349. https://doi.org/10.1515/cclm-2019-0657
- Dehhaghi M, Kazemi Shariat Panahi H, Guillemin GJ. Microorganisms, tryptophan metabolism, and kynurenine pathway: a complex ınterconnected loop ınfluencing human health status. Int J Tryptophan Res 2019; 12: 1178646919852996. https://doi.org/10.1177/1178646919852996
- Ghardallou M, Mtiraoui A, Ennamouchi D, et al. Bullying victimization among adolescents: Prevalence, associated factors and correlation with mental health outcomes. PLoS One 2024; 19: e0299161. https://doi.org/10.1371/journal.pone.0299161
Copyright and license
Copyright © 2026 The Author(s). This is an open access article distributed under the Creative Commons Attribution License (CC BY), which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is properly cited.









