Abstract
Background. Siblings of children with autism spectrum disorder (ASD) are at increased risk of psychosocial difficulties due to altered family dynamics and parental stress. However, the mechanisms linking ASD severity, parental psychopathology, and sibling outcomes remain unclear. This study aimed to identify determinants of psychosocial problems among siblings of children with ASD using a family-systems framework and structural equation modeling (SEM).
Methods. A case–control study was conducted with 67 siblings of children with ASD (ASD-Sibs) and 67 siblings of typically developing children (TD-Sibs), aged 6–18 years. ASD severity was rated using the Childhood Autism Rating Scale (CARS). Sibling depression, anxiety, and emotion regulation were assessed using the Child Depression Inventory (CDI), Screen for Child Anxiety Related Emotional Disorders (SCARED), and Cognitive Emotion Regulation Questionnaire (CERQ). Parents completed the Child Behavior Checklist (CBCL), Beck Depression and Anxiety Inventories (BDI, BAI), and Family Assessment Device (FAD). SEM was used to examine predictors of sibling psychosocial outcomes.
Results. ASD-Sibs reported significantly higher depressive and anxiety symptoms than TD-Sibs. SEM revealed that maternal depression and general family functioning were significant predictors of sibling depression, anxiety, and behavioral problems. ASD severity indirectly influenced sibling outcomes through maternal depression and anxiety. Positive reappraisal emerged as a protective factor against anxiety.
Conclusions. Maternal psychological well-being and family functioning are key determinants of psychosocial adjustment among ASD-Sibs. Autism severity affects siblings indirectly via maternal psychopathology, underscoring the importance of holistic, family-centered interventions to promote resilience in families of children with ASD.
Keywords: autism spectrum disorder, siblings, psychosocial adjustment, maternal depression, maternal anxiety, family functioning, structural equation modeling
Introduction
The family unit serves as a critical developmental context for children, offering both a primary socialization environment and a secure base.1 However, within a family systems framework, individual challenges can significantly impact overall family functioning.2 The presence of a child with autism spectrum disorder (ASD), for instance, profoundly alters family dynamics, affecting not only the child but also all family members due to its pervasive developmental impacts.3
Parents of children with ASD often assume roles beyond typical parenting and become de facto special educators.4 They navigate complex behavioral challenges5, strive to meet the needs of other family members, and frequently contend with social isolation and stigma6,7. Personal time for self-care and social engagement is often significantly limited.8
Siblings of children with ASD (ASD-Sibs) also experience unique challenges related to their sibling’s condition, including behavioral issues, communication difficulties, and the demand for continuous support.9 Reduced parental attention, a common experience for ASD-Sibs, may lead to increased attention-seeking behaviors and internalizing problems. The implicit expectation to provide support can also generate feelings of burden and stress.10 Difficulties in sibling relationships, potentially marked by complex social interactions and conflicts, may also extend to peer relationships, exacerbating stress levels.10,11
Existing literature consistently indicates that ASD-Sibs exhibit a heightened vulnerability to diminished psychological well-being and lower psychosocial functioning compared to siblings of typically developing children (TD-Sibs).12 Recent research, although focused on identifying risk factors, often reports inconsistent findings due to the heterogeneous nature of ASD and the unique characteristics of families, highlighting the complexity of this area. Among the key variables warranting investigation, family stress stands out. Autism families (families of children with ASD) experience unique daily stressors, which are associated with increased rates of parental anxiety and depression.13 Parental stress14 and general family distress15 are positively correlated with siblings’ psychosocial problems. Some research suggests that increased family stress may directly impact siblings’ distress more than relational difficulties with their autistic sibling.14 Conversely, other studies have found no significant association between sibling adjustment and maternal stress or family support.16
Another complex area is the relationship between ASD severity and sibling outcomes. While challenging behaviors in children with ASD are consistently linked to sibling outcomes17, the direct impact of autism severity is less clear, likely due to the spectrum’s wide phenotypic variability. Some studies report a positive association between symptom severity and sibling adjustment difficulties18, while others find no significant relationship19. This inconsistency underscores the need to identify mediating variables that clarify how ASD severity influences sibling psychosocial problems.
Emotion regulation skills are also crucial for stress management, conflict resolution, and maintaining emotional balance. Despite their importance, few studies have explored the contribution of emotion regulation skills to psychosocial problems in ASD-Sibs. One intervention program noted improved relationships between autistic siblings and those with enhanced emotion regulation skills.20 Given that ASD-Sibs frequently encounter chronic and emotionally demanding family environments, examining their cognitive emotion regulation strategies offers a meaningful way to understand both vulnerability and resilience pathways.
Gender significantly shapes sibling relationships21, and its broad influence on psychosocial development within the context of ASD is also well-established. Sisters often report a stronger sense of responsibility towards their siblings with ASD22, whereas brothers may exhibit higher rates of emotional and conduct problems and peer difficulties16. Consequently, brothers of children with ASD may face more psychosocial challenges than sisters.23 However, conflicting evidence suggests that sisters may experience elevated anxiety and depression compared to brothers.24
Finally, birth order is another critical factor. Older siblings often show better psychological functioning than younger ones.25 This is hypothesized to occur because older siblings experience a period of typical family life before the full impact of ASD is felt, while younger siblings encounter these challenges from an earlier developmental stage.26 Thus, the influence of birth order on sibling understanding, expectations, and engagement warrants further investigation.
This study aimed to identify determinants contributing to psychosocial problems in ASD-Sibs, specifically investigating internalizing and externalizing problems from both sibling and parental perspectives. Predictor variables were categorized into three domains: child-related (autism severity, intelligence level), family-related (maternal and paternal depression/anxiety, household income, family functionality), and sibling-related (birth order, gender, cognitive emotion regulation skills).
Materials and Methods
Study design and participants
The study protocol was approved by the Ankara University Faculty of Medicine Ethics Committee (protocol number: 11-717-18). Written informed consent was obtained from all participants, and procedures adhered to the Declaration of Helsinki. Data were collected between November 2019 and April 2020.
This case-control study included 67 age- and sex-matched ASD-Sibs and TD-Sibs, along with their mothers and fathers. Eligible siblings were 6–18 years old and volunteered to participate. TD-Sibs had no prior psychiatric diagnoses. Exclusion criteria for both groups were ASD or intellectual disability, neurological/chronic illness, and institutional care.
Children with ASD were initially evaluated and ASD diagnoses were confirmed by experienced child psychiatrists and clinical psychologists based on DSM-V criteria. Study participation was announced to physicians at the Child and Adolescent Psychiatry and General Pediatrics clinics of our tertiary care center. Eligible families were referred to our clinic. Siblings and parents attended clinical interviews for the collection of information and sociodemographic data. Following preliminary evaluation, autism severity was rated with the Childhood Autism Rating Scale (CARS), after which siblings and parents completed questionnaires.
In the ASD-Sibs group, 3 siblings were excluded due to intellectual disability, 5 due to ASD, and 3 due to neurological/chronic illness; additionally, 9 families declined participation or did not complete the study forms, resulting in a final ASD-Sibs sample of 67. In the TD-Sibs group, 23 families declined participation and 7 children were excluded due to neurological/chronic illness in themselves or a sibling, resulting in a final TD-Sibs sample of 67.
To ensure developmental comparability, siblings were categorized as children (< 12 years: ASD-Sibs n = 26, TD-Sibs n = 27) and adolescents (≥ 12 years: ASD-Sibs n = 41, TD-Sibs n = 40) for subgroup analyses.
Measures
Sociodemographic information
A semi-structured interview form collected data on sibling, family, and autistic child sociodemographic attributes, including age, gender, parental education and employment, and household income (Table I).
|
a Student's t-test, b Chi-square test 1 p value for siblings under 12 years of age (child group), 2 p value for siblings aged 12 and older (adolescent group) SD: standard deviation. |
|||||
| Table I. Sociodemographic characteristics of groups. | |||||
| Variables |
Mean ± SD / n (%) |
Mean ± SD / n (%) |
|
||
| Sibling characteristics |
|
|
|
|
|
| Age a |
|
|
|
||
|
|
|
|
|||
| Gender b | |||||
| Female |
|
|
|
|
|
| Male |
|
|
|
|
|
| Parent characteristics | |||||
| Mother age a |
|
|
|
||
| Father age a |
|
|
|
||
| Mother’s education (year) a |
|
|
|
||
| Father’s education (year) a |
|
|
|
||
| Family characteristics | |||||
| Family type b, (nuclear) |
|
|
|
||
| Monthly family income b | |||||
| Low (≤330$) |
|
|
|
||
| Medium (330-1000$) |
|
|
|||
| High (>1000$) |
|
|
|||
Child autism severity
The Childhood Autism Rating Scale (CARS) was used to rate autism severity.27 CARS includes 15 items rated from 1–4 (with intermediate ratings), yielding a total score typically ranging from 15 to 60, where higher scores indicate greater autism severity. Turkish validity and reliability have been established, with high internal consistency (α = 0.95) and test-retest reliability (r = 0.98).28
Siblings’ self-report measures
Child Depression Inventory (CDI) is a self-report scale for depressive symptoms (6–18 years).29 The CDI consists of 27 items scored on a 0–2 scale (total score range: 0–54), with higher scores indicating greater depressive symptom severity. The Turkish adaptation demonstrated good internal consistency (α = 0.82).30
Screen for Child Anxiety Related Emotional Disorders (SCARED) is a 41-item self-report measure for childhood anxiety disorders.31 SCARED includes 41 items rated 0–2 (total score range: 0–82) and yields subscale scores for Panic/Somatic, Generalized Anxiety, Separation Anxiety, Social Anxiety, and School Avoidance; higher scores indicate greater anxiety. Its Turkish adaptation showed strong internal consistency (α = 0.91).32
Cognitive Emotion Regulation Questionnaire (CERQ) is a 36-item self-report assessing nine cognitive emotion regulation strategies following adverse events.33 Subscales (four items each) are maladaptive (Self-blame, Rumination, Catastrophizing, Blaming others) or adaptive (Acceptance, Putting into perspective, Positive refocus, Refocus on planning, Positive reappraisal). Each CERQ subscale comprises 4 items scored 1–5 (subscale score range: 4–20); higher scores indicate more frequent use of that strategy. Turkish validation yielded similar results, with subscale α ranging from 0.72 (Self-blame) to 0.83 (Catastrophizing).34
Parent-report measures
Child Behavior Checklist (CBCL 6-18): The 2001 version was used to assess behavioral/emotional problems.35 The CBCL contains 113 problem items rated 0–2 and yields syndrome scales and broadband Internalizing and Externalizing scales; results are typically reported as age- and sex-standardized T-scores (mean = 50, SD = 10), with higher scores indicating more problems. The Turkish version demonstrated good internal consistency for Internalizing (α = 0.87, r = 0.93), Externalizing (α = 0.90, r = 0.93), and Total Problems (α = 0.94, r = 0.93).36
Beck Depression Inventory (BDI) is a self-report measure of adult depression severity.37 The BDI consists of 21 items scored 0–3 (total score range: 0–63), with higher scores indicating more severe depressive symptoms. The Turkish adaptation showed good internal consistency (α = 0.84).38
Beck Anxiety Inventory (BAI) is a 21-item self-report for clinical anxiety.39 The BAI includes 21 items scored 0–3 (total score range: 0–63), with higher scores indicating greater anxiety severity. Its Turkish adaptation demonstrated excellent internal consistency (α = 0.95).40
Family Assessment Device (FAD) is a self-administered measure of family functioning based on the McMaster Model.41 The FAD comprises 60 items rated on a 4-point Likert scale and consists of seven subscales (Problem Solving, Communication, Roles, Affective Responsiveness, Affective Involvement, Behavior Control, General Functioning); higher scores reflect poorer family functioning. Turkish validation indicated subscale α values ranging from 0.62 to 0.90.42
Data analysis
Statistical analyses were conducted using SPSS 23.0 (Statistical Package for the Social Sciences), AMOS 23.0 statistical software, and R for bootstrap estimation. Continuous variables are presented as mean ± standard deviation (SD) when normally distributed and as median (Q1–Q3) when non-normally distributed; categorical variables are presented as number (%). Normality was assessed using the Shapiro–Wilk test and visual inspection of histograms and Q–Q plots. Pearson chi-square tests compared categorical variables. For continuous variables, Student’s t-test or Mann-Whitney U test was applied after confirming data normality. Pearson or Spearman correlation tests were used to assess relationships, and structural equation modeling (SEM) was used to identify determinants of sibling psychosocial problem scores.
In line with a family-systems framework, variables that were theoretically expected to influence sibling adjustment (autism severity, maternal and paternal depression and anxiety, general family functioning, and siblings’ cognitive emotion regulation) were initially entered into the SEM. Non-significant paths and parameters that weakened overall model fit were then trimmed stepwise, particularly in view of the relatively small sample size, yielding a final model that retained only theoretically meaningful and statistically supported predictors. In this process, paternal BDI and BAI were initially included but were removed from the final specification because their structural paths were non-significant and their inclusion did not improve overall model fit. Model fit was evaluated using χ², χ²/df, the Comparative Fit Index (CFI), the Normed Fit Index (NFI), and the Root Mean Square Error of Approximation (RMSEA). Model fit was considered acceptable when CFI and NFI were ≥ 0.90 and RMSEA ≤ 0.08, and indicative of good fit when CFI ≥ 0.95, RMSEA ≤ 0.05, and χ²/df ≤ 2. SEM findings were interpreted with caution, and a sensitivity analysis re-estimated the final model under a constrained specification in which no correlated residuals were allowed.
Effect sizes were interpreted according to Cohen’s guidelines: r = 0.20 for small, r = 0.50 for medium, and r = 0.80 for large effects.43 All analyses employed a two-tailed p-value of 0.05 for statistical significance.
Results
Demographics
Sociodemographic variables are presented in Table I. No significant differences were observed between ASD-Sibs and TD-Sibs regarding sibling (age, gender, number of siblings), parental (age, education level), and family (family type, household income) characteristics.
Normative comparisons in siblings
In the child group, ASD-Sibs exhibited significantly higher scores on the CDI (p < 0.001) and SCARED (p = 0.001) compared to TD-Sibs. However, no statistically significant differences were found between these groups on the CBCL Internalizing (p = 0.123) and Externalizing Problems (p = 0.419) subscales (Table II).
|
CERQ was administered to adolescents (≥12 years) only. Student's t-test, * p < 0.05, ** p < 0.01, *** p < 0.001. ASD: autism spectrum disorder; ASD-Sibs: siblings of children with ASD; TD-Sibs: siblings of typically developing children; CBCL: Child Behavior Checklist; CDI: Child Depression Inventory; CERQ: Cognitive Emotion Regulation Questionnaire; SCARED: Screen for Child Anxiety Related Emotional Disorders. |
||||||||
| Table II. Normative comparisons between sibling groups by age group (<12 years vs ≥12 years). | ||||||||
|
|
|
|||||||
|
|
Mean±SD |
|
|
|
Mean±SD |
|
|
|
| CDI |
|
|
|
|
|
|
|
|
| SCARED |
|
|
|
|
|
|
|
|
| Internalizing problems (CBCL) |
|
|
|
|
|
|
|
|
| Externalizing problems (CBCL) |
|
|
|
|
|
|
|
|
| CERQ Subscales | ||||||||
| Self-blame |
|
|
|
|
|
|
|
|
| Acceptance |
|
|
|
|
|
|
|
|
| Rumination |
|
|
|
|
|
|
|
|
| Positive refocus |
|
|
|
|
|
|
|
|
| Refocus on planning |
|
|
|
|
|
|
|
|
| Positive reappraisal |
|
|
|
|
|
|
|
|
| Putting into perspective |
|
|
|
|
|
|
|
|
| Catastrophizing |
|
|
|
|
|
|
|
|
| Other-blame |
|
|
|
|
|
|
|
|
Among adolescent siblings, ASD-Sibs reported significantly higher CDI scores than controls (p = 0.004), but no significant difference was observed in anxiety scores (p > 0.05) (Table II). Additionally, adolescent ASD-Sibs scored higher on both CBCL Internalizing (p = 0.01) and Externalizing Problems (p = 0.006) subscales compared to controls (Table II). CERQ subscale scores did not differ significantly between the groups (Table II). Fig. 1 shows the mean CBCL syndrome-scale T-scores in adolescent siblings (≥12 years). Compared with TD-Sibs, adolescent ASD-Sibs showed higher T-scores across several CBCL domains, with differences particularly evident in the broadband Internalizing and Externalizing scales, consistent with the group comparisons reported in Table II.
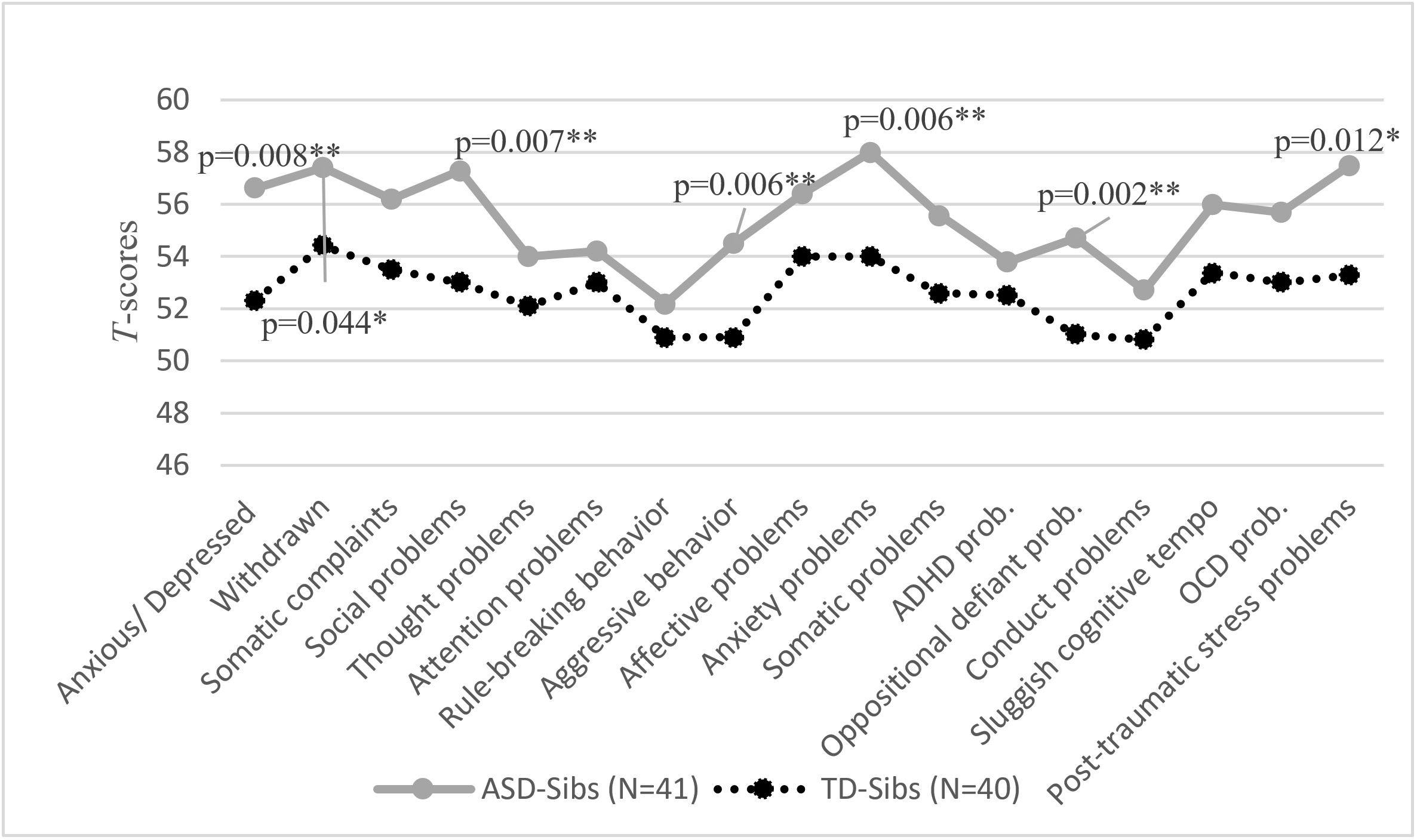
ADHD: attention deficit hyperactivity disorder; ASD-Sibs: siblings of children with ASD; OCD: obsessive compulsive disorder; TD-Sibs: siblings of typically developing children.
Clinical range percentages in siblings
Based on CDI cut-off scores, 13% of ASD-Sibs presented with mild depression, 3% with moderate, and 6% with severe depression. In contrast, 1% of TD-Sibs showed mild depression. For CBCL Internalizing Problems, 16% of ASD-Sibs were in the clinical range and 11% in the borderline range, while 5% of TD-Sibs were in the clinical range and 4% in the borderline range. Regarding CBCL Externalizing Problems, 9% of ASD-Sibs were in the clinical range and 3% in the borderline range, with only 1% of TD-Sibs falling into the borderline range.
Normative comparisons in parents and general family functioning
Mothers and fathers of children with ASD reported significantly higher depressive and anxiety symptoms compared to parents in the control group (Table III). Significant group differences in family functioning were found in Problem Solving (1.81 ± 0.57 vs. 1.48 ± 0.46; p < 0.001), Communication (1.74 ± 0.48 vs. 1.51 ± 0.4; p = 0.004), Affective Responsiveness (1.66 ± 0.47 vs. 1.51 ± 0.43; p = 0.049), and General Functioning (1.65 ± 0.47 vs. 1.35 ± 0.3; p < 0.001) domains. Other FAD subscale scores were comparable between groups (p > 0.05). All FAD subscale results are presented in Table III.
|
For BDI and BAI, values are presented as Mean ± SD for variables analyzed with Student’s t-test and as median (Q1–Q3) for variables analyzed with the Mann–Whitney U test. FAD subscale values are presented as Mean ± SD and compared using Student’s t-test. a Student’s t-test, b Mann-Whitney U Test, * p < 0.05, ** p < 0.01, *** p < 0.001. ASD: autism spectrum disorder; ASD-Pr: parents of children with ASD; BAI: Beck Anxiety Inventory; BDI: Beck Depression Inventory; FAD: Family Assessment Device; SD: standard deviation; TD-Pr: parents of typically developing children. |
||||
| Table III. Parent psychological distress (BDI, BAI) and family functioning (FAD) in ASD and control families. | ||||
|
|
|
|
|
|
| Mothers | ||||
| BDI |
|
|
|
|
| BAI |
|
|
|
|
| Fathers | ||||
| BDI |
|
|
|
|
| BAI |
|
|
|
|
| FAD subscale |
|
|
|
|
| Problem Solving |
|
|
|
|
| Communication |
|
|
|
|
| Roles |
|
|
|
|
| Affective Responsiveness |
|
|
|
|
| Affective Involve |
|
|
|
|
| Behavior Control |
|
|
|
|
| General Function |
|
|
|
|
Clinical range percentages in parents
Maternal BDI scores indicated that among mothers of children with ASD, 27% experienced mild, 19% moderate, and 3% severe depression; whereas in control mothers, these rates were 7% mild and 1% moderate. Maternal anxiety levels in the ASD group revealed 26% mild, 20% moderate, and 12% severe symptoms in the clinical range. For control mothers, 9% were in the mild, 8% moderate, and 1% severe clinical range.
Among fathers in the ASD group, 21% reported mild depression and 10% moderate depression. In the control group, 5% of fathers had mild and 3% moderate depressive symptoms. Paternal anxiety scores in the ASD group showed 21% in the mild, 11% moderate, and 7% severe clinical range, compared to 16% mild, 4% moderate, and 1% severe clinical range in control fathers.
Correlations
Correlations among the main study measures in the ASD-Sibs group are presented in Supplementary Table S1. Sibling outcomes (CDI, SCARED, CBCL Internalizing and Externalizing) were not significantly correlated with parental age, parental education, household income, autism severity (CARS), or the autistic child’s intelligence level (all p > 0.05). In contrast, maternal depressive and anxiety symptoms and poorer general family functioning were positively correlated with siblings’ psychosocial outcomes, whereas CERQ positive reappraisal showed an inverse association with sibling anxiety (Supplementary Table S1).
Gender and birth order comparisons
Regarding gender (33 girls, 34 boys), no statistically significant difference was observed in psychosocial problems between girls and boys in either age group (p > 0.05), except for anxiety scores (p = 0.001).
In birth order comparisons, younger siblings (n = 15) displayed numerically higher scores than older siblings (n = 47) on CDI (10.0 ± 8.6 vs. 8.9 ± 6.1; p = 0.790), SCARED (23.4 ± 13.2 vs. 21.8 ± 11.8, p = 0.64), Internalizing Problems (57.6 ± 7.7 vs. 53.2 ± 11.1, p = 0.161), and Externalizing Problems (51.6 ± 7.63 vs. 46.5 ± 10.8, p = 0.093). However, these differences were not statistically significant (p > 0.05).
Predictors of psychosocial problems in siblings of children with ASD
SEM was employed to investigate predictors of siblings’ psychosocial problems and to examine indirect effects. Potentially confounding demographic variables (age, gender, and family income) were controlled, and a confirmatory factor analysis supported the measurement model’s adequacy for SEM. The measurement model demonstrated good fit to the data (χ²(17) = 10.244, p = 0.893; χ²/df = 0.603; CFI = 1.000; NFI = 0.957; RMSEA = 0.000). Given the modest sample size (n = 67), these indices should be interpreted cautiously and considered alongside theoretical plausibility and a simple, theory-driven model specification.
Bootstrap-based parameter estimates (standard errors, 95% confidence intervals, z statistics, and p-values) for both direct and indirect effects are presented in Table IV (direct paths) and Supplementary Table S2 (indirect effects).
|
Columns include standardized (Std β) and unstandardized (B) coefficients with bootstrap SE and 95% CI. BAI: Beck Anxiety Inventory; BDI: Beck Depression Inventory; CARS: Childhood Autism Rating Scale; CBCL: Child Behavior Checklist; CDI: Child Depression Inventory; CERQ - Positive reap.: Cognitive Emotion Regulation Questionnaire—Positive reappraisal subscale; Ext. Prob.: CBCL Externalizing Problems; FAD–Gen.: Family Assessment Device—General Functioning; Int. Prob.: CBCL Internalizing Problems; SCARED: Screen for Child Anxiety Related Emotional Disorders. |
||||||||
| Table IV. Direct effects in final SEM (bootstrap estimates). | ||||||||
| Path (predictor → outcome) |
|
|
|
|
|
|
|
|
| CARS → BDI |
|
|
|
|
|
|
|
|
| CARS → BAI |
|
|
|
|
|
|
|
|
| FAD–Gen. → BDI |
|
|
|
|
|
|
|
|
| FAD–Gen. → BAI |
|
|
|
|
|
|
|
|
| FAD–Gen. → CDI |
|
|
|
|
|
|
|
|
| FAD–Gen. → SCARED |
|
|
|
|
|
|
|
|
| FAD–Gen. → Int. Prob. |
|
|
|
|
|
|
|
|
| FAD–Gen. → Ext. Prob. |
|
|
|
|
|
|
|
|
| BDI → CDI |
|
|
|
|
|
|
|
|
| BDI → SCARED |
|
|
|
|
|
|
|
|
| BDI → Int. Prob. |
|
|
|
|
|
|
|
|
| BDI → Ext. Prob. |
|
|
|
|
|
|
|
|
| BAI → SCARED |
|
|
|
|
|
|
|
|
| CERQ - Positive reap. → SCARED |
|
|
|
|
|
|
|
|
Indirect effects were evaluated using bootstrap confidence intervals, and results are reported to facilitate transparent interpretation of precision alongside point estimates.
Sensitivity analysis (model without correlated residuals): To address concerns regarding potential overfitting, we additionally estimated a more constrained specification in which no correlated error terms were allowed. As expected, this constraint resulted in poorer global fit (χ²(22) = 68.885, p < 0.001; χ²/df = 3.13; CFI = 0.104; NFI = 0.246; RMSEA = 0.180), likely reflecting shared variance among conceptually related outcomes and measurement-method overlap. We therefore report the constrained model fit transparently and interpret the final SEM findings primarily on the basis of theoretical coherence.
The SEM results (Fig. 2) indicate that maternal depression (0.25) and family general functioning (0.17) were positive predictors of sibling depression. For sibling anxiety, maternal depression (0.29) and maternal anxiety (0.16) were positive predictors, while positive reappraisal (-0.25) was a negative predictor. In terms of internalizing problems, maternal depression (0.17), maternal anxiety (0.18), and family general functioning (0.43) emerged as positive predictors. Finally, maternal depression (0.17) and family general functioning (0.51) were positive predictors for externalizing problems.
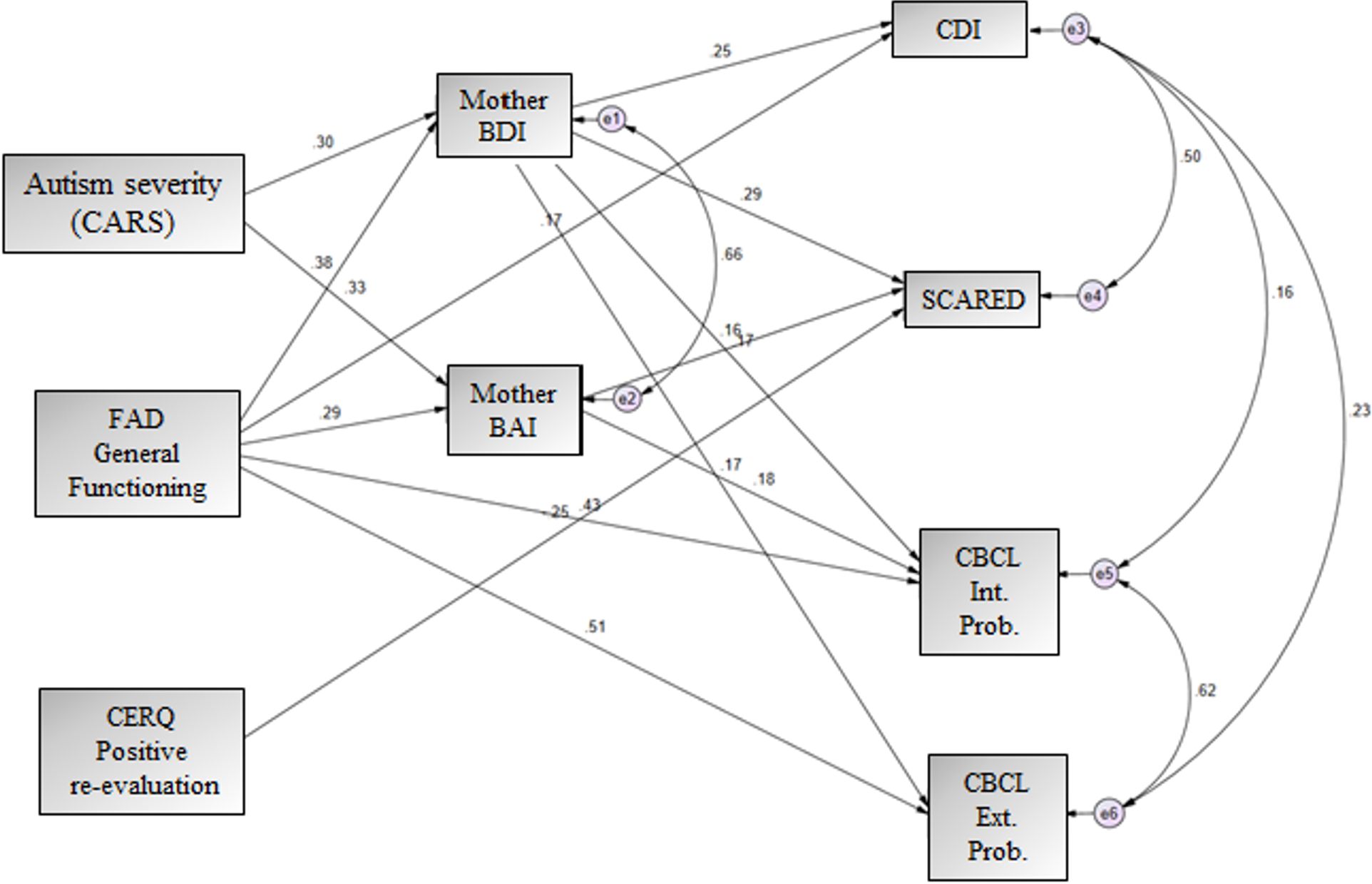
The model also revealed that autism severity positively predicted maternal depression (0.30) and maternal anxiety (0.33) but did not directly predict outcomes in ASD-Sibs. However, autism severity exerted an indirect effect on ASD-Sibs’ problems, mediated through maternal depression and anxiety. The indirect effects of autism severity on sibling outcomes were: depression = 0.076, anxiety = 0.285, internalizing problems = 0.185, and externalizing problems = 0.085.
Discussion
This study investigated various potential predictors of psychosocial problems in ASD-Sibs, including parental psychological well-being, family functioning, ASD symptom severity, and sibling characteristics.
A key finding from our SEM analysis was that maternal depression significantly predicted siblings’ psychosocial outcomes, with maternal anxiety symptoms specifically associated with higher sibling anxiety and internalizing problems. These results align with previous research demonstrating a strong link between parental psychological distress and sibling adjustment.14,44 This is further supported by meta-analytic evidence highlighting a robust association between maternal depressive symptoms and children’s internalizing, and externalizing problems, as well as general psychopathology.45,46 However, a contrasting study by Hesse et al. found that while parental stress correlated with sibling challenges, this relationship did not fully explain adjustment issues when other parent-related factors were considered.47 This discrepancy might stem from their focus on parental stress rather than clinical depression. While stress may indicate the severity of situational challenges, depressive symptoms reflect a more profound emotional impact on mothers.
Furthermore, our model revealed that the impact of autism symptom severity on sibling outcomes was fully mediated by maternal depressive and anxiety symptoms. This suggests that ASD severity does not directly influence sibling psychosocial problems but rather acts through its effect on maternal psychological well-being. This mediation is consistent with the results of Meyer et al., who found that maternal depression was the primary mediator of siblings’ problems.48 This outcome provides clarity to the mixed findings often reported in the literature regarding the direct relationship between ASD severity and sibling adjustment.
Another significant finding was the notable effect of general family functioning on sibling problems. Our model confirms that robust family functioning is a vital determinant of sibling outcomes, aligning with prior research indicating that family factors, such as cohesion and a positive family climate, are associated with better sibling psychological well-being.49 Collectively, our results strongly support the existing literature emphasizing family functionality and parental psychological well-being as primary predictors of siblings’ psychosocial challenges.14,15
Regarding initial group comparisons, self-report measures indicated that ASD-Sibs, particularly in the child group, reported higher levels of depression and anxiety compared to TD-Sibs. This was an unexpected finding, as adolescents typically show greater susceptibility to internalizing problems. This could suggest that younger ASD-Sibs may struggle more with processing and adjusting to family changes, leading to heightened distress24, potentially due to less developed cognitive coping mechanisms or a more immediate and less filtered perception of family stressors compared to adolescents. However, it is important to note that only a minority of ASD-Sibs met clinical diagnostic criteria, implying that while they experience elevated problems, it is more accurate to identify those at heightened risk and their specific vulnerabilities rather than to universally conclude that all ASD-Sibs experience clinical-level psychosocial issues.
Our study also explored the influence of birth order and gender on the psychological well-being of ASD-Sibs. Consistent with a recent meta-analysis by Park et al.50 and previous literature25,26, our findings specifically indicated that younger ASD-Sibs were more vulnerable to internalizing problems than older ones. This heightened vulnerability in younger siblings may stem from their developmental context, often being born into a family already navigating significant burdens, whereas older siblings might have experienced a period of typical family life before the full impact of ASD was felt, potentially fostering greater psychological resilience.26
Furthermore, our findings are in line with previous reports suggesting that birth order and developmental timing may shape vulnerability among ASD-Sibs. Consistent with a recent meta-analysis by Park et al. and earlier studies, younger siblings appeared more prone to internalizing difficulties than older ones, possibly because they were born into a family system that was already under the strain of caring for a child with ASD.25,26,50 In this context, older siblings may have benefited from a period of relatively typical family functioning before the onset or recognition of ASD-related challenges, which could support greater psychological resilience. However, our sample size did not allow for adequately powered tests of more fine-grained interactions between birth order, age-spacing, and gender, and future studies with larger cohorts are needed to clarify these patterns.
Conversely, younger female ASD-Sibs with wider age-spacing were more likely to develop anxiety symptoms. This is consistent with the literature indicating that typically developing sisters of individuals with ASD often report higher negative emotionality than their male counterparts51, and our results further suggest that specific birth order and age-spacing dynamics for younger females may exacerbate this predisposition to anxiety. These findings collectively highlight that while general demographic factors like age and gender influence adjustment, a finer-grained analysis of birth order and age-spacing reveals distinct pathways of vulnerability to specific internalizing problems within the ASD-Sib population.
While overall emotion regulation strategies did not differ between groups, our SEM analysis revealed a crucial finding: positive reappraisal emerged as a significant negative predictor of sibling anxiety. This suggests that siblings who frequently employ positive reappraisal – reframing negative events in a more positive light or focusing on potential positive outcomes – experience lower levels of anxiety. This finding aligns with the broader literature on emotion regulation, which emphasizes adaptive cognitive strategies in mitigating psychological distress.52 For ASD-Sibs, facing unique and ongoing family stressors, the ability to find positive meaning or growth in challenging situations may serve as a vital protective factor against anxiety. This highlights the importance of fostering such adaptive cognitive strategies in interventions aimed at supporting the mental health of ASD-Sibs.
Finally, our findings imply that autism families may face difficulties in problem-solving, communication, and overall general family functioning compared to families with typically developing children. Effective communication and problem-solving skills are crucial for family resilience and for modeling adaptive coping strategies in children.14
Strengths, limitations, and directions for future research
This study contributes significantly to understanding predictors of psychosocial problems in ASD-Sibs within a Turkish context. Key strengths include the use of both self- and parent-reports (from both mothers and fathers), a carefully matched control group, and a relatively homogeneous sample of children with ASD. Additionally, the separate analysis of child and adolescent sibling groups, despite the broad age range, enhances precision and allows for developmental considerations.
Despite these strengths, several methodological limitations warrant consideration. First, the SEM was conducted only in the ASD-Sibs group (n = 67), which is a modest sample size for multivariable modeling. Although SEM can be applied to smaller samples in simple, theory-driven models, parameter estimates and global fit indices may be unstable and potentially optimistic, increasing the risk of overfitting—particularly when model refinement is guided by modification indices. In a sensitivity analysis, the model fit worsened when correlated residuals were not allowed, suggesting that global fit may be sensitive to model constraints and shared variance among conceptually related outcomes. Therefore, the SEM findings should be interpreted with caution and require replication in larger and independent samples, ideally with external validation, before strong generalizable inferences are made. Second, the study was not powered to test more fine-grained interactions between birth order, age-spacing, and gender, and larger samples will be needed to clarify these more specific patterns of vulnerability. Third, we did not investigate certain unexamined confounders in ASD-Sibs, such as subthreshold autism-like traits, or school-related adjustment issues (e.g., bullying, academic performance). In addition, maternal psychological well-being, identified as a key mediator in our model, may be influenced by unmeasured factors like coping skills and social support. Future research would benefit from incorporating these variables to gain a more comprehensive understanding. Finally, the study’s primary focus on psychopathology might restrict broader conclusions regarding overall well-being and adaptive functioning.
Future research should therefore adopt a more holistic approach, considering a wider range of individual and social characteristics that foster resilience or vulnerability within the family system, moving beyond a sole focus on psychopathology. Larger and more diverse samples will also be important to test the robustness and generalizability of the SEM pathways identified in this study.
Conclusions
In summary, our study provides robust evidence that maternal psychological well-being and family functionality are primary determinants of psychosocial problems in ASD-Sibs. A crucial insight from our structural equation model is that ASD severity does not directly impact sibling problems but rather exerts its influence indirectly, with maternal depressive and anxiety symptoms acting as key mediators. Furthermore, we identified a significant finding regarding cognitive emotion regulation: the frequent use of positive reappraisal strategies was associated with lower anxiety levels in siblings, suggesting a potential protective factor.
These results underscore the necessity of a family systems perspective when evaluating the mental health needs of children with ASD and their siblings. Early identification and intervention for family dysfunction, particularly addressing maternal psychological distress, can significantly prevent mental health problems across family members. Developing tailored social support interventions for autism families, especially mothers, holds substantial public health and preventive medicine importance, strengthening family resilience and promoting overall well-being.
Acknowledgements
The authors thank all participating families for their valuable contribution to this study.
Ethical approval
The study was approved by Ankara University Faculty of Medicine Ethics Committee (date: June 25, 2018, number: 11-717-18). Written informed consent was obtained from all participants, and procedures adhered to the Declaration of Helsinki.
Source of funding
The authors declare the study received no funding.
Conflict of interest
The authors declare that there is no conflict of interest.
References
- Wang Y. Influence of early family nurturing environment on children’s psychological and emotional social development. Iran J Public Health 2023; 52: 2138-2147. https://doi.org/10.18502/ijph.v52i10.13852
- Johnson BE, Ray WA. Family systems theory. In: Shehan CL, editor. Encyclopedia of Family Studies. 1st ed. Hoboken, NJ: Wiley; 2016: 1-5. https://doi.org/10.1002/9781119085621.wbefs130
- Karst JS, Van Hecke AV. Parent and family impact of autism spectrum disorders: a review and proposed model for intervention evaluation. Clin Child Fam Psychol Rev 2012; 15: 247-277. https://doi.org/10.1007/s10567-012-0119-6
- Ingersoll B, Dvortcsak A. Including parent training in the early childhood special education curriculum for children with autism spectrum disorders. Top Early Child Spec Educ 2006; 26: 179-187. https://doi.org/10.1177/02711214060260030501
- Zaidman-Zait A, Mirenda P, Duku E, et al. Examination of bidirectional relationships between parent stress and two types of problem behavior in children with autism spectrum disorder. J Autism Dev Disord 2014; 44: 1908-1917. https://doi.org/10.1007/s10803-014-2064-3
- Quintero N, McIntyre LL. Sibling adjustment and maternal well-being: an examination of families with and without a child with an autism spectrum disorder. Focus Autism Other Dev Disabl 2010; 25: 37-46. https://doi.org/10.1177/1088357609350367
- Cantwell J, Muldoon O, Gallagher S. The influence of self-esteem and social support on the relationship between stigma and depressive symptomology in parents caring for children with intellectual disabilities. J Intellect Disabil Res 2015; 59: 948-957. https://doi.org/10.1111/jir.12205
- Hutton AM, Caron SL. Experiences of families with children with autism in rural New England. Focus Autism Dev Disabil 2005; 20: 180-189. https://doi.org/10.1177/10883576050200030601
- Watson L, Hanna P, Jones CJ. A systematic review of the experience of being a sibling of a child with an autism spectrum disorder. Clin Child Psychol Psychiatry 2021; 26: 734-749. https://doi.org/10.1177/13591045211007921
- Mokoena N, Kern A. Experiences of siblings to children with autism spectrum disorder. Front Psychiatry 2022; 13: 959117. https://doi.org/10.3389/fpsyt.2022.959117
- Caner N, Sezer Efe Y, Vural B, Ertaş EB. Peer relationships, emotional and behavioral problems in siblings of children with autism spectrum disorder. Child Youth Serv Rev 2024; 156: 107372. https://doi.org/10.1016/j.childyouth.2023.107372
- Quatrosi G, Genovese D, Amodio E, Tripi G. The quality of life among siblings of autistic individuals: a scoping review. J Clin Med 2023; 12: 735. https://doi.org/10.3390/jcm12030735
- Suthar S, Sethi S. Prevalence of depression, anxiety, and stress among parents of children with autism spectrum disorders in North India: a cross-sectional study. Taiwan J Psychiatry 2025; 39: 23-27. https://doi.org/10.4103/tpsy.tpsy_8_25
- Giallo R, Gavidia-Payne S. Child, parent and family factors as predictors of adjustment for siblings of children with a disability. J Intellect Disabil Res 2006; 50: 937-948. https://doi.org/10.1111/j.1365-2788.2006.00928.x
- Benson PR, Karlof KL. Child, parent, and family predictors of latter adjustment in siblings of children with autism. Res Autism Spectr Disord 2008; 2: 583-600. https://doi.org/10.1016/j.rasd.2007.12.002
- Hastings RP. Behavioral adjustment of siblings of children with autism engaged in applied behavior analysis early intervention programs: the moderating role of social support. J Autism Dev Disord 2003; 33: 141-150. https://doi.org/10.1023/a:1022983209004
- Walton KM. Risk factors for behavioral and emotional difficulties in siblings of children with autism spectrum disorder. Am J Intellect Dev Disabil 2016; 121: 533-549. https://doi.org/10.1352/1944-7558-121.6.533
- Jones EA, Fiani T, Stewart JL, Sheikh R, Neil N, Fienup DM. When one sibling has autism: adjustment and sibling relationship. J Child Fam Stud 2019; 28: 1272-1282. https://doi.org/10.1007/s10826-019-01374-z
- Tomeny TS, Barry TD, Bader SH. Are typically-developing siblings of children with an autism spectrum disorder at risk for behavioral, emotional, and social maladjustment? Res Autism Spectr Disord 2012; 6: 508-518. https://doi.org/10.1016/j.rasd.2011.07.012
- Kennedy DE, Kramer L. Improving emotion regulation and sibling relationship quality: the more fun with sisters and brothers program. Fam Relat 2008; 57: 567-578. https://doi.org/10.1111/j.1741-3729.2008.00523.x
- Jensen AC, Whiteman SD, Fingerman KL, Birditt KS. “Life Still Isn’t Fair”: Parental differential treatment of young adult siblings. J Marriage Fam 2013; 75: 438-452. https://doi.org/10.1111/jomf.12002
- Cridland EK, Jones SC, Stoyles G, Caputi P, Magee CA. Families living with autism spectrum disorder: roles and responsibilities of adolescent sisters. Focus Autism Dev Disabil 2016; 31: 196-207. https://doi.org/10.1177/1088357615583466
- Walton KM, Ingersoll BR. Psychosocial adjustment and sibling relationships in siblings of children with autism spectrum disorder: risk and protective factors. J Autism Dev Disord 2015; 45: 2764-2778. https://doi.org/10.1007/s10803-015-2440-7
- Orsmond GI, Seltzer MM. Adolescent siblings of individuals with an autism spectrum disorder: testing a diathesis-stress model of sibling well-being. J Autism Dev Disord 2009; 39: 1053-1065. https://doi.org/10.1007/s10803-009-0722-7
- Petalas MA, Hastings RP, Nash S, Lloyd T, Dowey A. Emotional and behavioural adjustment in siblings of children with intellectual disability with and without autism. Autism 2009; 13: 471-483. https://doi.org/10.1177/1362361309335721
- Tomeny TS, Barry TD, Bader SH. Birth order rank as a moderator of the relation between behavior problems among children with an autism spectrum disorder and their siblings. Autism 2014; 18: 199-202. https://doi.org/10.1177/1362361312458185
- Schopler E, Reichler RJ, DeVellis RF, Daly K. Toward objective classification of childhood autism: Childhood Autism Rating Scale (CARS). J Autism Dev Disord 1980; 10: 91-103. https://doi.org/10.1007/BF02408436
- İncekaş Gassaloğlu S, Baykara B, Avcil S, Demiral Y. Validity and reliability analysis of Turkish version of Childhood Autism Rating Scale. Turk Psikiyatri Derg 2016; 27: 266-274.
- Kovacs M. The Children’s Depression, Inventory (CDI). Psychopharmacol Bull 1985; 21: 995-998.
- Öy B. Çocuklar için depresyon ölçeği: geçerlik ve güvenirlik çalışması. Türk Psikiyatri Derg 1991; 2: 132-6.
- Birmaher B, Brent DA, Chiappetta L, Bridge J, Monga S, Baugher M. Psychometric properties of the Screen for Child Anxiety Related Emotional Disorders (SCARED): a replication study. J Am Acad Child Adolesc Psychiatry 1999; 38: 1230-1236. https://doi.org/10.1097/00004583-199910000-00011
- Karaceylan F. Çocuklarda anksiyete bozukluklarını tarama ölçeği geçerlik ve güvenirlik çalışması [specialty thesis]. Kocaeli: Kocaeli University, Faculty of Medicine; 2004.
- Garnefski N, Kraaij V, Spinhoven P. Negative life events, cognitive emotion regulation and emotional problems. Personal Individ Differ 2001; 30: 1311-1327. https://doi.org/10.1016/S0191-8869(00)00113-6
- Tuna E, Bozo Ö. The Cognitive Emotion Regulation Questionnaire: Factor structure and psychometric properties of the Turkish version. J Psychopathol Behav Assess 2012; 34: 564-570. https://doi.org/10.1007/s10862-012-9303-8
- Achenbach TM. Child behavior checklist for Ages 6-18. Burlington, VT: University of Vermont; 2001. https://doi.org/10.1037/t47452-000
- Erol N, Şimşek Z. Okul çağı çocuk ve gençler için davranış değerlendirme ölçekleri el kitabı. Ankara: Mentis Yayıncılık; 2010.
- Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Arch Gen Psychiatry 1961; 4: 561-571. https://doi.org/10.1001/archpsyc.1961.01710120031004
- Hisli N. Beck Depresyon Envanteri’nin üniversite öğrencileri için geçerlik ve güvenirliği. Turk Psikol Derg 1989; 7: 3-13.
- Beck AT, Epstein N, Brown G, Steer RA. An inventory for measuring clinical anxiety: psychometric properties. J Consult Clin Psychol 1988; 56: 893-897. https://doi.org/10.1037/0022-006X.56.6.893
- Ulusoy M, Şahin NH, Erkmen H. Turkish version of the Beck Anxiety Inventory: psychometric properties. J Cogn Psychother 1998; 12: 163-172.
- Epstein NB, Baldwin LM, Bishop DS. The McMaster Family Assessment Device. J Marital Fam Ther 1983; 9: 171-180. https://doi.org/10.1111/j.1752-0606.1983.tb01497.x
- Bulut I. Aile Değerlendirme Ölçeği El Kitabı. Ankara: Özgüzeli Yayınları; 1990: 1-50.
- Cohen J. A power primer. Psychol Bull 1992; 112: 155-159. https://doi.org/10.1037/0033-2909.112.1.155
- Koukouriki E. Psychological distress among Greek parents of children with an autism spectrum disorder: Is there a link to anxiety symptoms in neurotypical offspring? Eur Psychiatry 2021; 64: S615. https://doi.org/10.1192/j.eurpsy.2021.1635
- Ivanova MY, Achenbach TM, Turner LV. Associations of parental depression with children’s internalizing and externalizing problems: meta-analyses of cross-sectional and longitudinal effects. J Clin Child Adolesc Psychol 2022; 51: 827-849. https://doi.org/10.1080/15374416.2022.2127104
- Goodman SH, Rouse MH, Connell AM, Broth MR, Hall CM, Heyward D. Maternal depression and child psychopathology: a meta-analytic review. Clin Child Fam Psychol Rev 2011; 14: 1-27. https://doi.org/10.1007/s10567-010-0080-1
- Hesse TL, Danko CM, Budd KS. Siblings of children with autism: predictors of adjustment. Res Autism Spectr Disord 2013; 7: 1323-1331. https://doi.org/10.1016/j.rasd.2013.07.024
- Meyer KA, Ingersoll B, Hambrick DZ. Factors influencing adjustment in siblings of children with autism spectrum disorders. Res Autism Spectr Disord 2011; 5: 1413-1420. https://doi.org/10.1016/j.rasd.2011.01.027
- Black K, Lobo M. A conceptual review of family resilience factors. J Fam Nurs 2008; 14: 33-55. https://doi.org/10.1177/1074840707312237
- Ran Park H, Moon H, Sil Kim Y, Karkar Esperat TM, Lee J. A meta-analysis on adjustment difficulties in siblings of children with and without autism spectrum disorder. Int J Spec Educ 2023; 38: 16-33. https://doi.org/10.52291/ijse.2023.38.2
- Hamama L, Gaber S. Seeing the siblings: gender differences in emerging-adult siblings of individuals with autism spectrum disorder. Res Dev Disabil 2021; 108: 103829. https://doi.org/10.1016/j.ridd.2020.103829
- Shaheen H, Rashid S, Aftab N. Dealing with feelings: moderating role of cognitive emotion regulation strategies on the relationship between cyber-bullying victimization and psychological distress among students. Curr Psychol 2023; 42: 29745-29753. https://doi.org/10.1007/s12144-023-04934-1
Copyright and license
Copyright © 2026 The Author(s). This is an open access article distributed under the Creative Commons Attribution License (CC BY), which permits unrestricted use, distribution, and reproduction in any medium or format, provided the original work is properly cited.